Nearly 17,000 people may have died after taking hydroxycholoroquine during the first wave of Covid-19, according to a study by French researchers.
The anti-malaria drug was prescribed to some patients hospitalized with Covid-19 during the first wave of the pandemic, “despite the absence of evidence documenting its clinical benefits,” the researchers point out in their paper, published in the February issue of Biomedicine & Pharmacotherapy.
Now, researchers have estimated that some 16,990 people in six countries — France, Belgium, Italy, Spain, Turkey and the U.S. — may have died as a result.
That figure stems from a study published in the Nature scientific journal in 2021 which reported an 11 percent increase in the mortality rate, linked to its prescription against Covid-19, because of the potential adverse effects like heart rhythm disorders, and its use instead of other effective treatments.
Researchers from universities in Lyon, France, and Québec, Canada, used that figure to analyze hospitalization data for Covid in each of the six countries, exposure to hydroxychloroquine and the increase in the relative risk of death linked to the drug.
In fact, they say the figure may be far higher given the study only concerns six countries from March to July 2020, when the drug was prescribed much more widely.
Hydroxychloroquine gained prominence partly due to French virologist Didier Raoult who had headed the Méditerranée Infection Foundation hospital, but was later removed amid growing controversy.
It was also considered something of a “miracle cure” by the then-U.S. President Donald Trump, who said: “What do you have to lose? Take it.”
And why? I still don’t fully understand what made Trump and the GOP decide to deny vaccines publicly (while often taking vaccines privately) and to turn every medical decision into a toxic political decision based on misinformation. Why was this in their interest? Once they started down this path, they just kept doubling down, leading to the ridiculously unqualified and dangerous Florida State Surgeon General currently in power.
It’s exactly why Rand Paul invested in hydroxychloroquine early on in the early months of COVID, and then regularly attacked Dr Fauci…as the good doctor was bad for Brillohead’s bottom line.
I think it’s a combination of things. It brews mistrust of experts, education, science, and medicine, which keeps people afraid. It’s a cult in that way, you must trust the leader and exclude information that might potentially prove them wrong. By putting in a mistrust of one area of expert, it can be extended to others as well, cementing that only the in group can be trusted.
By denying that people are dying, they make people distrust reports of people dying. When people do get sick, they wait or take ineffective ‘treatments’, which then overtax the hospital facilities if/when the person actually goes in for real treatment – and then the cult leaders can say that the hospital system is failing and can’t save you, only dear leader can.
But ultimately, I think they simply don’t care. As you say, they privately take the vaccines and have top flight health care. Everyone else is less than a pawn on the board to them.
At this point on the right the tail wags the dog. These memes are coming from somewhere and being picked up by people looking around down the Q and other right wing rabbit holes. The Republican leadership has little in the way of actual leadership. First it was Limbaugh and company but now it’s faceless, nameless internet bot farms setting their agenda. They can’t hold on to power without pandering to this shit and they are more afraid of losing power than killing their own supporters.
There’s little leadership in our politics. Few Democrats supported gay marriage until public polling showed a majority in favor. If that had been the case earlier in our history how long would it have taken for civil rights laws to be enacted or interracial marriage to be legal. We didn’t get to 50% in favor of interracial marriage until the late 80s! I realize you can’t be too far off public opinion and get elected, but leaders should be leading public opinion, not following it. Consensus can be created if people with good writing and oratorical skills get out there and make the case. Of course that means risking your access to power if you don’t succeed and that right there is the big problem we face in our politics.
Remember, it’s all part of Putin’s plan to undermine democracy. Part of that is to undermine the trust in any institutional authority. As soon as Covid hit, they realized it was easy to spread lies and made up stories, and they did. Eventually, it pitted some people against other people, which is exactly the goal. And when a mass of people are distrustful of government all the grifters realize they can get viewers by fanning the flames. So it spreads around and feds on itself. And it worked! If some people die, who cares?
Echoing Randy Ellicott & Houndentenor. Republicans intentionally sow so much distrust against doctors and research that they can promote quacks into their ranks without consequence.
it was in their interest because these people gain power by making other people afraid of anything and everyone. It was in their interest because these people gain power by making other people not trust respectable and respected authorities. It was in their interest because fear, doubt, confusion, And the politics of resentment are always in the interests of authoritarians, conmen, and grifter.
Evangelicals (the MAGAt base) quite literally worship a genocidal deity. Extend that fantasy into their nearly hermetically sealed reality and voila, we have a cult with a full on death wish.
Politics because the CDC and the “Democratic appointed” Fauci had to be opposed by GOP and for no other reason. Well, yes, because Trump had no idea how to act as President.
See, the problem was that they didn’t follow all of TFG’s advice and drink bleach and stick UV light in their butts after taking the hydroxychloroquine. /s
Republicans’ successful sowing of distrust towards science and doctors during the pandemic is the biggest consequence. When President Obama successfully led the creation of the H1N1 vaccine, no one blinked. But Trump and his like-minded lackeys lied and lied and lied about the vaccine that many Republican voters trust a rando podcaster or anti-vax preacher on the street more than peer-reviewed research.
And while these anti-vaxxers scam their viewership and rake in the $$, they take the vax behind the scenes.
Touting quack remedies instead of effective treatment for a disease that can kill you, or leave you seriously disabled for long stretches, is not the finest re-election tactic–especially when your opponent is urging his voters to get highly effective vaccines.
Touting quack remedies instead of effective treatment for a disease that can kill you, or leave you seriously disabled for long stretches, is not the finest re-election tactic–especially when your opponent is urging his voters to get highly effective vaccines.
Like all people who put their feelings before the facts, that value their feelings / dislikes / hates over medical science, Ladapo is convinced only he is correct on these things no matter what or how hard people try to explain things to them. They refuse to hear what they don’t want to. In the case of Ladapo his pay check requires him to be against the medical science, approved medical facts, and accepted best practices of the majority of medical providers. Hugs. Scottie
“We’ve seen this pattern from Dr. Ladapo that every few months he raises some new concern and it quickly gets debunked,” said Ashish Jha, dean of Brown University’s public health school who led the White House’s national coronavirus response. “This idea of DNA fragments — it’s scientific nonsense. People who understand how these vaccines are made and administered understand that there is no risk here.”
Florida’s health department did not respond to questions about whether Ladapo’s new stance would affect vaccine access for the state’s patients, or whether his decision to repeat debunked claims could create doubts about other routine vaccinations. Scott Rivkees, a DeSantis appointee who preceded Ladapo as Florida surgeon general, called Wednesday’s announcement “surprising and disappointing” and at odds with settled science.
Grateful to live in a state where Big Pharma does not dictate health policy recommendations. Thank you @FLSurgeonGen Dr. Ladapo for standing up for scientific integrity. https://t.co/M9IwUsJV6X
I feel sad for the regular people in Florida being used as a pawn by the Florida government to create a batshit crazy talking point for the GQP to exploit their ignorance. It’s gotten people killed and will continue to do so as covid spreads.
Florida is an extremely fragile state, with inevitable disaster looming. We live on the beach. 5 weeks ago, they just had 365 trackloads of sand per day x 7 days to refurbish the dunes in our tiny area (maybe 1/4 mile) and one week later half of the sand was already gone. 3 million just washed out to sea. No climate change here folks -nothing to see. High tides with wind can easily wash across the back streets on the Canal in Indian Rocks Beach. They use water here like it is an endless resource, allowing the freshwater aquifier to be depleted as water demand from urban areas and unsustainable agricultural practices continually increase and cause salt water intrusion. Hard to fathom really.
She channels Humpty Dumpty, who says to Alice, “When I use a word, it means just what I choose it to mean—neither more nor less.” Pushaw, like Humpty, has a whimsical approach to language and meaning, and does not let herself be overly bothered with reality… which does lead to tragic fatal falls.
Especially, in the quote in the picture of the article, he says “when the vaccines are known to be contaminated with foreign DNA”… no, dumbass. It’s mRNA, not DNA. Ribonucleic, not dioxyribonucleic. Big difference.
Yesterday Ladapo called for banning COVID vaccines due to “DNA integration,” a claim that was immediately ridiculed by vaccine experts and Ladapo’s own DeSantis-appointed predecessor in Florida.
So this is the crazy nutcase that Tildeb used to justify anti-trans hate. He is the Florida Surgeon General, handpicked by DeathSantis because of his anti-covid vaccine stance. He was given the job even though not qualified, and DeathSantis tried to force the state university to hire him at a huge sum of money. He refused to answer questions asked him by the Florida legislature and lied to them when forced to answer. He was part of the demon seed doctor’s team that scammed maga people by charging them huge fees for an online consultation, then prescribed Ivermectin to cure or prevent covid. It has been well proven that Ivermectin doesn’t do anything to cure or prevent covid. He has been soundly mocked by the scientific and medical communities. Remember if DeathSantis is elected to the presidency this is the type of people he hires. Below I will post the first part of the Wikipedia entry on him. Hugs. Scottie
JosephLadapoJoseph Abiodun Ladapo (born December 16, 1978) [1] is the surgeon general of Florida. [2] He has attracted attention for spreading misinformation on COVID-19 and promoting vaccine hesitancy. [
DeSantis’ Florida surgeon general Dr. Joseph Ladapo says covid mRNA vaccines “the Anti-Christ of all products… That’s so wrong, you know, it’s just complete disrespect to the human genome and the importance of protecting it and preserving it, and that is our connection to God.” pic.twitter.com/r1aGzHsBqz
mRNA, of course, is messenger molecules telling some of your immune cells to make specific antibodies. They don’t mess with DNA, they don’t get into your ova or sperm, they just wash out of your body within a few days. That’s what they were telling him when “They talked about a bunch of other things” that he didn’t understand.
The biggest thing about the new mRNA technology is getting the mRNA to survive long enough to make any proteins. The cells have a zillion RNAses waiting to chew up improper RNA not tagged with the exact signal for temporary protection. It has been nearly 20 years since I was a bench researcher handling RNA, and I still remember what a PITA it was to handle.
She is one of the people who claim to know more and be more moral than everyone else so she / them get to tell the rest of us how we must live and how our schools should be run. The article below shows how unqualified these people are to tell others how to live their lives. These people are simply self entitled ego driven people who feel entitled to rule over how others live, while often not living that way themselves. I won’t be coloring this one, too much in it is triggering to me.
Randy was visiting us the other day and we touched a bit on my abuse. For something realted. I told them something I had not told before. By the time I was 7 during my adoptive parents parties with their friends, I would be set / perched on the counter with all the booze and mixers and would be required to fix drinks for the people. They would come to me and hand me their glass, tell me what they wanted, I would make the drink and hand it back. If I did the job correctly and everyone left happy, I was rewarded but if anyone complained I was disciplined. Often right then and painfully humiliated. Sometimes I would have to stand at the counter and wait on the people playing cards, watching for their drinks to get low and offering to refill them. I learned to never let an empty glass go unaddressed. Needless to say, I did not go into detail and it was a brief mention.
A former Pennsylvania lieutenant governor candidate and outspoken voice in the conservative “parental rights” school movement has been charged with punching a teenager while hosting an underage drinking party at her Bucks County home in September.
Clarice Schillinger, 36, is facing criminal charges of assault, harassment and furnishing minors with alcohol during her daughter’s birthday party, according to the case filed in late October. Her attorney has denied all charges and said she will fight them in court.
Schillinger made an unsuccessful run for lieutenant governor as a Republican last year and has played an instrumental role in a political action committee that has poured more than $800,000 into Pennsylvania school district races since 2021. The PAC has focused on supporting school board candidates who opposed COVID-19 lockdowns and argue left-wing ideologies are invading the education system.
In the recent criminal case, Schillinger is accused of punching a partygoer several times in the face during a series of alleged outbursts by drunken adults at her home on Liz Circle in Doylestown, according to an affidavit of probable cause.
The documents state that during the event — which started Sept. 29 and went past midnight — Schillinger’s then-boyfriend allegedly grabbed a 16-year-old by the neck for intervening in a fight between the couple and hit a 15-year-old in the face during an argument over football. According to the allegations in court papers, her intoxicated mother also punched the older teen in the eye and chased him around the kitchen island. Police said they had cellphone recordings of some of these reported events.
To escape the unruly adults, several minors started making their way out of the home, even as Schillinger ordered them to stay, court documents allege.
Cellphone footage showed that as the teens gathered in the foyer Schillinger lunged toward one partygoer before others began restraining her. That individual told police Schillinger struck him three times with a closed fist but that he wasn’t injured, according to the affidavit.
Schillinger had been throwing a 17th birthday party for her daughter that night, hosting about 20 teens in her basement, where there was a bar stocked with New Amsterdam vodka and Malibu Bay Breeze rum, police wrote in the affidavit. In addition to supplying the underage group with alcohol, she allegedly poured liquor for the teens, asked them to take a shot with her and played beer pong with them, witnesses later told authorities.
State law makes it illegal to serve or allow minors to drink alcohol.
One of the teen’s parents called police early the morning of Sept. 30 to report the assaults and the underage drinking at Schillinger’s home. Investigators interviewed multiple teens who had attended the party, the affidavit states.
This wasn’t the first time police visited Schillinger’s home — which she’s been renting since the spring — for reports of an underage party, according to court documents.
Emergency dispatch data provided by the Bucks County Emergency Service Division logged at least four different calls at the address.
Buckingham Township police responded to a noise complaint call and possible underage party at Schillinger’s home on Sept. 24, the weekend before the birthday party, according to 911 data and court records.
Police reported in one affidavit spotting a number of beer cans strewn around the property and street that night. They also saw about 20 teens dart into the home and, when they tried speaking with Schillinger, found her to be “intoxicated and uncooperative,” the affidavit states.
Authorities responded to another noise complaint at Schillinger’s home involving “intoxicated subjects” just after midnight on Sept. 29, though an affidavit says police only made contact with Schillinger’s then-boyfriend, Shan Wilson, that night.
Schillinger is scheduled for a late January preliminary hearing. Her mother, Danette Bert, and Wilson were charged with assault and harassment in connection with the party, but those charges were withdrawn when they pleaded guilty to disorderly conduct in early December, court records show.
In an email, Schillinger said that her case had been dropped and suggested Wilson, whom she described as an “angry ex boyfriend,” was behind the accusations. However, online court records show the case is still active, and a spokesman for the Bucks County District Attorney’s Office said Wednesday that the charges are not being dismissed.
Schillinger has not responded to a request for further comment, including why she believes the charges against her were dropped.
While Wilson did contact the USA Today Network about the incident, the affidavit against Schillinger did not include any statements from him and relied instead on the testimony of teenage witnesses and the cellphone footage.
“Ms. Schillinger has dedicated her life to public service,” Schillinger’s attorney Matthew Brittenburg said in an emailed statement Wednesday. “Additionally, she has always been a law abiding citizen. Ms. Schillinger looks forward to the opportunity to defend against these allegations.”
Who is Clarice Schillinger?
Dissatisfied with school closures that followed the coronavirus pandemic in 2020, Schillinger created a political committee to help fund school board candidates who made strict adherence to in-person education their top campaign promise.
That PAC, Keeping Kids In School, focused more closely to school districts near Schillinger’s former home in Ambler, Montgomery County, by giving out thousands of dollars to smaller PACs backing slates of candidates running on an “open schools” platform.
Bucks County venture capitalist and Central Bucks parent Paul Martino took notice of Schillinger’s PAC before the municipal primary in May 2021, and the two created Back To School PA later that summer.
Martino initially put up $500,000 of his own money for Back To School PA to disburse $10,000 checks to local school board races across the state.
Schillinger told the conservative news organization Broad+Liberty after that year’s election that Back To School saw an “incredible win” with 113 of 182 candidates supported by the PAC winning elections.
Back To School took credit for flipping at least six school districts in that story, including Pennridge and Quakertown Community school districts in Bucks County; Harrisburg City in Dauphin County; Hempfield in Lancaster County; Palmyra in Lebanon County; and Southeastern in York County.
The PAC also gave $10,000 to Bucks Families for Leadership, which was an earlier PAC Martino created and funded backing Republican candidates in the 2021 Central Bucks school board race.
Three of the five Central Bucks Republicans that ran in 2021 made it onto the board, but this year’s municipal election saw Democrat candidates sweep five seats and take a 6-3 majority.
While Schillinger’s original PAC and Back To School were described as bipartisan and focused on the single-issue of school closures by her and Martino, most of the candidates endorsed were Republican and often opposed to other pandemic mitigations like requiring masks in schools.
Schillinger threw her hat in the ring for public office in 2022 joining eight other candidates in the Republican primary for lieutenant governor. Schillinger finished fourth, gaining over 148,000 votes of the 1.2 million cast for that office.
Schillinger announced that Back To School PA would be going national during a July 25, 2022, episode of 1210 WPHT’s The Dom Giordano Program.
“Back To School USA is really going to be focused on putting candidates in place that will put our children and their education first,” Schillinger said. “Right now, we are not doing that. We are more focused on these woke and gender ideas.”
A website for the national PAC, created in October 2021, is no longer publicly accessible.
Martino told Lehigh Valley News in September that Back To School USA was “more of an idea right now” but indicated Schillinger was still involved in a fundamental way.
He declined to comment on the charges against Schillinger but wrote in an email this week that Back To School USA “never got off the ground” because other projects took priority last year.
These laws are not based on medical science nor on any evidence of the conspiracies to turn cis kids into trans kids. That doesn’t happen any more than straight kids get turned gay by seeing a rainbow flag or reading a book with LGBTQIA characters. No these laws are based on bigotry and religious doctrines. How many times do you hear anti-trans people say god doesn’t make mistakes, so you have to be the gender of your body. But they said the same thing about people being gay decades ago, that people couldn’t be born gay because god did make mistakes. Guess what, it is not a mistake to be gay if you are gay and it is not a mistake to be trans if you identify as a gender different from what is showing between your legs. It is ignorance, hate, bigotry, and religious indoctrination masquerading as fake concern for “the children”. Hugs. Scottie
“Transgender children should receive equal treatment under the law. Parents should have the right to make the most fundamental decisions about how to care for their children,” Winmill said in his ruling.
“Every family wants what is best for their children, and families who love and accept their transgender youth are no different,” Li Nowlin-Sohl, senior staff attorney for the ACLU’s LGBTQ & HIV Project said in a statement. “These dangerous efforts to control our bodies and our families threaten the well-being of trans youth, the strength of our communities, and the ability of every family to determine what’s best for their child.”
“This victory is significant for Idaho transgender youth and their parents,” one advocate said.
A federal court ruled on Tuesdaythat an Idaho law prohibiting doctors from providing transgender minors with access to gender-affirming care is likely unconstitutional and blockedthe law from taking effect. The gender-affirming healthcare ban, which was originally planned to go into effect on January 1, would have made providing puberty blockers and hormone therapies to transgender youth a felony.
“This victory is significant for Idaho transgender youth and their parents, and will have an immediate positive impact on their daily lives,” Leo Morales, executive director of the ACLU of Idaho, said in a statement.
Judge B. Lynn Winmill of the U.S. District Court for the District of Idaho heldthat Idaho’s anti-trans law likely violated the Due Process Clause and the Equal Protection Clause under the 14th Amendment.
“Transgender children should receive equal treatment under the law. Parents should have the right to make the most fundamental decisions about how to care for their children,” Winmill said in his ruling.
RELATED STORY
“Every family wants what is best for their children, and families who love and accept their transgender youth are no different,” Li Nowlin-Sohl, senior staff attorney for the ACLU’s LGBTQ & HIV Project said in a statement. “These dangerous efforts to control our bodies and our families threaten the well-being of trans youth, the strength of our communities, and the ability of every family to determine what’s best for their child.”
Another plaintiff in the lawsuit, Pam Poe, a 15-year-old trans girl, “struggled with depression, anxiety and self-harm” before receiving gender-affirming care which “greatly improved” her mental health. If the gender-affirming healthcare ban went into effect, her and her family would have considered leaving the state.
“This judicial decision is a much-needed ray of hope for trans people amid a years-long onslaught against their rights to access health care and ability to navigate the world around them,” Morales said in a press release. “Everyone should be free to live and thrive in their authentic identity, which means transgender people should not be shut out of accessing medically sound health care.”
Idaho is one of 22 states that have restricted or banned transgender youth from accessing gender-affirming care, according to the Movement Advancement Project(MAP). In a recent report, MAP described the gender-affirming healthcare bans as part of a “war against LGBTQ people in America and their very right and ability to openly exist.” While many of these bans have been temporarily blocked by the courts, the U.S. Court of Appeals for the Sixthand EleventhCircuits have reversed lower court injunctions, allowing bans in Kentucky, Tennessee and Alabama to go into effect.
Research by the Trevor Projectshows that debates around anti-trans bills negatively affect transgender and nonbinary youth’s mental health and a majority of those trans youth (55 percent) said anti-trans bills “very negatively” affected their mental health. Gender-affirming healthcare bans don’t just hurt transgender and nonbinary people, but also affect the health and well-being of LGBTQ+ adults, according to a Human Rights Campaign poll. The poll found that 8 in 10 LGBTQ adults said that the bans made them feel less safe and “worsen[ed] harmful stereotypes, discrimination, hate and stigma.”
A MESSAGE FROM TRUTHOUT’S EXECUTIVE DIRECTOR
For 22 years, Truthout has been a platform for new and daring ideas, uplifting voices and producing trailblazing, award-winning journalism. The stories we’ve published over the last two decades have been read by tens of millions of people and inspired the conversations and actions that are necessary for social change.
But to continue publishing meaningful, powerful, inspiring journalism, we still need to raise $65,000 before December 31st — and for a limited time, any donation you make will be matched, dollar for dollar.
This fundraiser is our most important drive, and the perfect time to make your end-of-year donation. Your support is both vitally needed, and deeply appreciated, so if you’re in a position to give, please make your tax-deductible gift today.
Gender-affirming care is not mutilating kids genitals. That is male circumcision in babies. Gender-affirming care is not a sudden thing where an 8 or 9 year old kid walks in to a doctor’s office and tells the people at the desk they need puberty blockers, hormones, and sexual reassignment surgery scheduled for next week please. Oh and do you have any apps / phone games I can download?
Gender affirming care saves lives! That is a fact! Gender affirming care is careful medical exams and phycological assessment. The care for younger kids includes letting them dress as the gender they identify as and to wear the hair and accessories that gender uses. Only as the child nears puberty or it is determined to be starting, are they given puberty blockers, which are safe and reversible. They are well studied and used for a very long time worldwide. If the kid decides they do not want to transition, they can stop the puberty blockers and they enter puberty as they would have before.
Only when the older teen has lived as the gender they identify as for a while and nears adulthood is any surgery discussed, and it is very rare to only in cases of great need is it considered before the age of 18. Normal age of sexual reassignment surgery is early 20s.
Why are these anti-trans bills clearly discriminatory? Because they only deny puberty blockers, hormones, and surgery to trans kids and for transitioning. The laws state that they can be used on cis kids, including the often used breast surgery to enlarge female cis kid’s boobies, normally around 16. Also other body changing surgeries for cis kids are allowed like rhinoplasty which is nose reshaping surgery. Also cis kids at very young teen years are allowed to have their ears reshaped for looks. See how the laws target trans kids and are not based on medical science? If puberty blockers were so harmful and non-reversible, why are they allowed for cis kids then? Think on it? It is like the anti-sodomy laws in Texas found to be illegal. They said anal sex between a male and female were OK, but anal sex between two males were illegal. Same with oral sex, it is OK between a male and female but illegal between two females or two males. WTF! See the bigotry and hate? That is why the courts ruled the laws were illegal. Hugs. Scottie
Myriam and Cameron in NCLR’s “Healthcare is Caring” PSA.Photo: Screenshot
The National Center for Lesbian Rights (NCLR) is combating anti-trans misinformation with a campaign that’s all about love and care.
Last month, the non-profit public interest law firm, which advocates for LGBTQ+ rights, launched its “Healthcare is Caring” campaign with a short PSA directed by Emmy-nominated filmmaker Zen Pace. The clip features the voices of trans teens reading letters to their parents describing their experiences of coming out and the impact their parents’ support had on them.
The ACLU is trying to stop a ban from going into effect.
It ends with a poignant and timely message: “The thing our kids have always needed is care.”
“This film is special to me because not only does it touch my community, but it helps put forward a much more accurate story of these families that simply doesn’t exist out there,” Pace said in a statement. “It gives space to these parents; it’s a gift from their children.”
According to The Drum, NCLR’s “Healthcare is Caring” campaign was developed with the help of public relations and marketing consultancy firm Edelman. The firm’s data and intelligence division conducted a study on how misinformation about gender-affirming care spreads online. It found that a disproportionately small number of voices have driven anti-trans discourse, leading to a wave of state laws and local restrictions that have banned gender-affirming care for young people and severely limited trans people’s ability to exist openly and safely in the public sphere.
NCLR has been combating such legislation. The firm has challenged laws banning gender-affirming care for minors in Alabama, Florida, and Kentucky. After the Sixth U.S. Circuit Court of Appeals upheld state bans in Kentucky and Tennessee, the NCLR filed a petition on November 3 urging the Supreme Court to review the decision. The American Civil Liberties Union, the ACLU of Tennessee, and Lambda Legal have also asked the Supreme Court to review the Tennessee decision. If the justices agree to hear the case, it would be the first time a case involving gender-affirming care has ever come before the court.
As part of the “Healthcare” is Caring campaign, NCLR is urging supporters to sign an open letter calling on elected leaders to ensure equal access to gender-affirming care — which is recognized by every major American medical association as evidence-based, safe, and often necessary for the treatment of gender dysphoria. The letter calls on elected officials to put an end to both legal bans and the false narratives characterizing this lifesaving health care as “child abuse.”
The campaign’s hub on NCLR’s website also features more info about the families featured in the PSA, including the full text of their letters.
“The families in our campaign, like so many other families with transgender children, are proof that helping transgender youth get medically needed care can enable them to lead happy and successful lives,” NCLR legal director Shannon Minter said in a statement. “Still, many legislators continue to push harmful policies that prevent these young people from getting the healthcare they need and deserve. We’re working to take action against these bills and show the politicians behind them that transgender youth and their families are not alone.”
Thanks to Ten Bears for the link. This is for my readers in Oregon and surrounding areas. What is wrong with republican voters that they keep voting for wack job crazy people for state and federal office. These people love conspiracies and endorsing them. They prefer fantasy rather than facts or science. I guess it comes from believing in the myths about tRump instead of the facts, just as they ignore reality for a literal bible infallibility. There are videos at the link above. Hugs. Scottie
A pair of Oregon Republican legislators, state Sens. Dennis Linthicum and Kim Thatcher, have appeared on multiple QAnon-affiliated and far-right shows to promote a lawsuit they are involved with that claims the federal government inflated COVID-19 numbers.
The lawsuit was filed in federal district court in Oregon in March 2022 by Linthicum, Thatcher, and naturopathic doctor Henry Ealy, who has spread COVID-19 misinformation. It claims that the federal government “failed to ensure and/or willfully manipulated data being collected, analyzed, and published,” causing “a significant hyperinflation of COVID-19 case, hospitalization, and death counts,” which they claim was used to defraud taxpayers of at least $3.5 trillion in public funds between 2020 and 2022. (The claim that COVID-19 cases were overcounted during the pandemic is dubious.)
The plaintiffs want to empanel a special grand jury and present “evidence of alleged crimes relating to the federal government’s handling of the COVID-19 pandemic.” The case was dismissed in November 2022, but the group appealed to the 9th U.S. Circuit Court of Appeals.
In recent weeks, Linthicum — who is also a former treasurer of the Oregon Republican Party — and Thatcher went on several programs affiliated with the QAnon conspiracy theory to promote the case.
On November 17, Linthicum and Thatcher appeared on Right Now with Ann Vandersteel, which is hosted by a known QAnon supporter who also promotes the extreme ideology of the sovereign citizenmovement. During the interview, Vandersteel praised them and Ealy as “incredible” for “com[ing] together to adjudicate the problem that apparently our government seems incapable of doing” with the “COVID fraud.”
Linthicum also pushed COVID-19 misinformation during the appearance, falselyclaiming that “face masks don’t work.”
Later that month, Linthicum, Thatcher, and Ealy sat for an interview with QAnon influencer Michael Jaco in which Thatcher called for others to “duplicate” this legal effort “all over the United States, whether people want to go to their counties or whether they could go to their — you know, the state grand jury or even do their own federal grand jury,” and Linthicum criticized what he called “COVID fraud.”
Linthicum also claimed that people are “redefining … what a vaccine is, what a vaccine isn’t,” and Thatcher pushed election misinformation, calling for people to “overwhelm whatever cheating might be out there and get their votes in.”
Video file
Video Player
00:00
09:54
CitationFrom the November 29, 2023, edition of Unleashing Intuition Secrets, streamed on Rumble
In early December, Linthicum appeared on The Tina Peters Show, which streams on the QAnon-affiliated Badlands Media Rumble channel.
During the interview, Linthicum claimed that there was an “anxiety drive” and that authorities were “fearmongering with mediocre science and uncertainty, scaring the public into getting the vaccine and increasing uptake rates,” calling it “criminal fraud.”
Host Tina Peters praised Linthicum and the other plaintiffs, calling them “brave souls” and saying the lawsuit is “a solution to taking back our country.”
Video file
Video Player
00:00
05:49
CitationFrom the December 4, 2023, edition of Badlands Media’s The Tina Peters Show, streamed on Rumble
During the interview, Linthicum seemingly disputed death tolls reported in the news, saying, “There’s this disconnect between what we’re seeing on the news — the nightly, you know, scrolling numbers: ‘175,000 people died today because of coronavirus’ and whatever. And it’s like, you know, in the United States of America, I know there’s only been eight cases and we’re already talking vaccines. And then, you know, there were 17 cases and then there’s videos of people dropping dead.”
Video file
Video Player
00:00
04:41
CitationFrom the December 2, 2023, edition of Sons of Liberty Media, streamed on Bitchute
During the interview, Linthicum promoted the lawsuit, pushed false claims that the 2020 presidential election had been significantly impacted by election fraud, and promised Icke that he would come back on the show “whenever you please.” Icke praised Linthicum as “honorable” and thanked him for “all the work that you’re doing over there trying to expose” the “COVID fraud” and “election fraud as well.”
Linthicum and Thatcher’s appearances on the QAnon-affiliated shows are the latest example of an ongoing partnership between anti-vaccine and QAnon figures, with right-wing anti-vaccine figures using QAnon shows to spread COVID-19 and vaccine-related misinformation and conspiracy theories.
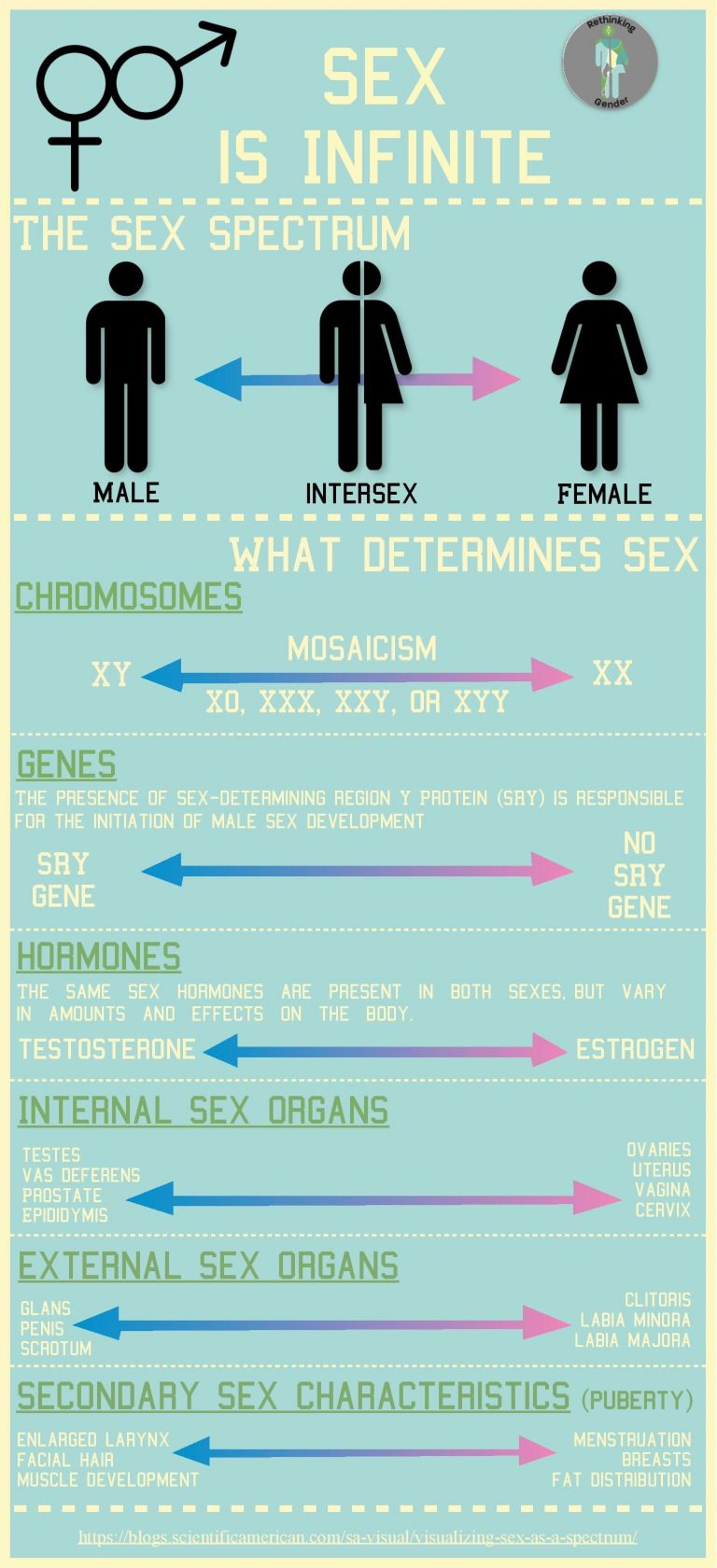
Thanks to Ali for the link. As I have pointed out, science has proven that sex is a spectrum / sliding scale from mostly male to mostly female chemical make up of a being. There is not one simple fixed point at which a person is male or female because biological sex is not binary. Yes it is hard for some people to grasp because for centuries the idea was if it dangles it is male and if not it is female, and if it dangles only a little because it is too short then cut it off so you can raise it as female. Again proven not to work. So what do we mean by male or female is a spectrum? Well because it is a spectrum or sliding scale a person can have a little or a lot of the chemical mix of DNA, chromosomes, enzymes, switches, and other things only scientist can understand or pronounce to look like one side of the slider but inside be all over the slider to the other side of it. The article is about birds, but the article makes it clear this same thing has been found in a lot of other animal species. And guess what? Humans are just another animal species. Hugs. Scottie
The bilaterally gynandromorphic green honeycreeper. Credit: John Murillo
A zoologist from New Zealand has spotted an extremely rare half female, half male bird while on holiday in Colombia.
The wild green honeycreeper (Chlorophanes spiza) has distinct green female plumage on its left and blue male plumage on its right.
This rare specimen is an example of bilateral gynandromorphy – a condition in which one side of an organism has male characteristics, and the other female.
“Many birdwatchers could go their whole lives and not see a bilateral gynandromorph in any species of bird. The phenomenon is extremely rare in birds, I know of no examples from New Zealand ever,” says Professor Hamish Spencer of the University of Otago, New Zealand.
***Video at link above, I am unable to post it here on WordPress***
Play Video
Short video of a bilaterally gynandromorphic Green Honeycreeper near Manizales, Colombia, 20 May 2022. Credit: John Murillo
Spencer was holidaying in Colombia when amateur ornithologist, John Murillo, pointed out the uncommon colouration.
“It is very striking; I was very privileged to see it,” Spencer says.
The finding, which is documented in a report in the Journal of Field Ornithology, is the 2nd example of gynandromorphism in this species in more than 100 years, and the 1st of a living bird.
The bilaterally gynandromorphic green honeycreeper. Credit: John Murillo
According to Spencer, the photographs of the bird are “arguably the best of a wild bilateral gynandromorphic bird of any species ever”.
Gynandromorphism occurs in a large number of groups of animals but is most often reported in species which display strong sexual dimorphism, including insects (especially butterflies), crustaceans, spiders, lizards, snakes and rodents.
Sexes of the same sexually dimorphic species display different physical characteristics. This makes it easier to distinguish gynandromorphism, where one side of the animal looks very distinct from the other.
The bilaterally gynandromorphic green honeycreeper. Credit: John Murillo
“This particular example of bilateral gynandromorphy – male one side and female the other – shows that, as in several other species, either side of the bird can be male or female,” says Spencer.
“The phenomenon arises from an error during female cell division to produce an egg, followed by double-fertilisation by two sperm.”
This error causes the egg cell to have two nucleuses: one with a Z chromosome and the other with a W chromosome. These are the sex chromosomes in birds, whereas in humans they are X and Y.
The bilaterally gynandromorphic green honeycreeper. Credit: John Murillo
Then, each of the two nucleuses are fertilised by a separate sperm. As a result, one side of the bird has female cells (ZW chromosomes) and the other has male cells (ZZ chromosomes).
The researchers observed the bird between October 2021 and June 2023. Its behaviour largely matched those of other green honeycreepers – except for one major difference.
“In general, it avoided others of its species, and the others also avoided it; it seems unlikely, therefore, that this individual would have had any opportunity to reproduce,” they concluded.
“When I woke up, I discovered that I had been shot 30 times.”
Abderrahman Al Zeghel, a 14-year-old Palestinian child and the youngest prisoner released in the Hamas-Israel hostage exchange, sustained deadly head injuries after Israeli forces assaulted him while he was buying bread in occupied East Jerusalem’s Silwan.
Despite undergoing multiple surgeries, he now lives with “half a skull” and faces health issues preventing a return to normal life.
Israeli law doesn’t permit the imprisonment of children under 14 and instead enforces house arrests as a form of punishment.
As I previously reported, the ADF first filed its lawsuit in May 2021 and lost in US district court in September 2021 before losing again before the 9th Circuit Court of Appeals in September 2022. According to Brian Tingley’s resume, he’s led seminars on “authentic manhood” and “true masculinity.” Before that, he wrote and produced commercials for car dealerships, bingo halls, and county fairs. As I’ve reported many times over the years, ex-gay torture therapists often end up rejecting their work and coming out as gay themselves. And sometimes, they are arrested for sexually assaulting their clients.
Then there are the ones that are busted trolling online for gay sex, such as the nationally prominent therapist caught cruising Manhunt in 2018 as HotNHairy72. The Alliance Defending Freedom, whose lead attorney was once House Speaker Mike Johnson, has advocated for criminalizing homosexuality in the United States and has provided free legal support to foreign groups seeking the same in their own countries.
The Supreme Court on Monday rejected a Christian therapist’s free speech challenge to a Washington state ban on so-called conversion therapy aimed at changing a child’s sexual orientation or gender identity.https://t.co/ZiLMCeHH0G
Given that Justices Thomas, Alito, and Kavanaugh all voted to hear a challenge to the constitutionality of Washington's ban on so-called "conversion therapy," we know that no other justice wanted to take up this case. Gorsuch's vote is somewhat surprising. https://t.co/EWShUNArYI
My sexuality is not a “debate.” It’s a fact of life, just as a straight person’s sexuality is a fact of life. Just because these religious whack jobs are too stupid to understand that should not be my problem.
No one is stopping him from saying his beliefs. What they are doing is preventing him from imposing them on others through the guise of medical treatment and accepting money for it. You can also believe massage cures cancer but you can not put out a medical shingle and take money for curing cancer through massage.
Or you can believe blood letting cures depression but you can not charge for this as a medical treatment. We have medical standards based on science.
The more right wingers are silenced, the louder they get all over social media and right wing tv and radio. They are the only silenced people who are deafeningly loud.
Brian Tingley, a licensed marriage and family counselor, said the law violates his free speech rights under the Constitution’s First Amendment because the government is seeking to dictate what he says.
No, the gov’t is still letting you “say” anything you want. They are regulating how you conduct your business so that you don’t harm your patients.
What the government is saying they are not going to pay for the mumbo jumbo via Medicaid or approve it for reimbursement by insurance companies. It is not banned, you just have to pay for the religious practice yourself.
Exactly right. The courts have long recognized that commercial speech is more subject to regulation than other kinds of speech. Tingley et al. are trying to argue that it is religious speech in a commercial context. Um, sorry, no.