It did not take long for the facts to come out and totally debunk the latest anti-trans conspiracy TERF talking point but sadly the planned damage was already underway. This woman who worked at a clinic claims she sees kids forced to transition and gives a screed that reinforced every right-wing talking point, which have been proven wrong time and time again by medical and demographic studies. Turns out this exposé was of course a fake bunch of lies by an anti-trans person trying to sabotage medical care for trans kids during the legislative session. If you want the facts, read the article. Hugs
I have spend most of my day on this. My morning was spend helping a confused elderly couple with their clogged printer head because they have not printed in years and now want to do so. I got it to start working by repeatedly doing the head clean, yet they did not even know where they paper went in the machine. They were laying it on top, wonder it worked at all. So after I came home and ate, I took my medications and came down with a very severe allergic reaction that is only now trying to abate. As any long time follower will know I have life threatening allergies and even though I felt I could handle it due to the entire body response including the genital area Ron lost his composure demanding I take more Benadryl than I had and thought I should to stop the cascade of reaction. But regardless as the extra Benadryl would only make me more tired and sleepy, I gave in. Must keep peace in the home / family. So I am very tired, irritable, hurting, and have to go back tomorrow morning to help the couple I was helping today as they screwed everything up. So I will leave comments open and try to monitor them. If they go from facts and feelings to fringe stuff, conspiracies, and already debunked myths that are countered by the best practices approved by the majority of medical communities then I will shut them off. Best wishes. Hugs
Jamie Reed’s story is being pushed by the worst of the worst anti-trans voices on the internet. I dig point-by-point through her claims and show how they undermine her conclusions.
Please support my independent reporting and activism on transgender legislation by subscribing. You help me keep this going and keep people informed.
On February 9th, a former case worker at the Washington University’s Transgender Center at St. Louis Children’s Hospital released an article in The Free Press alleging widespread wrongdoing among clinicians in treating transgender patients. Within hours, right wing sources across the internet were carrying her story. Anti-trans organization Genspect, which has advocated for bans on gender affirming care up to the age of 25 years old, announced an interview with her live. The Republican attorney general of Missouri announced an investigation. Vernadette Broyles, an attorney who has tried several cases to overturn transgender policies in schools and who advised Ron DeSantis on the Don’t Say Gay law, was tapped to represent her. This has all of the markings of a manufactured controversy similar to Project Veritas’ Planned Parenthood Fetal Tissue, and similar groups are lining up behind this story.
We know that this story has been held back for at least two weeks and judging from the timing of the anti-trans bills heard in Missouri, the speed in which right wing outlets carried the story, and its release in the middle of the legislative season with the most attacks on transgender rights and healthcare in history, it’s hard not to see this as entirely planned. Delving into Jamie Reed’s allegations and story makes it clear that she is not an ideologically neutral individual on the care and respect of transgender people. Her statements and omissions reveal a clear ideological bias, and the organizations and representation she has chosen to work with contradict her claim that she “supports transgender people.”
Throughout her story, she frequently misgenders her patients. In fact, I am not aware of a single case where she genders her trans patients correctly. Out of the thousand or so patients she has seen, she only references a half dozen specific anecdotes of what she relays as poor experiences for transgender youth patients – anecdotes I will cover in detail. Even in these anecdotes, she often omits long term net harm. She leaves out the stories of what must be the rest of the thousand patients who, as we have seen in numerous testimony in hearings this year, saw their mental and physical health improve dramatically. Ultimately, she calls for stopping gender affirming care for trans youth – something that would result in actual harm and death to this patient population.
She is not a doctor, a psychologist, a psychiatrist, and does not have direct medical diagnostic experience with patients. She is a case worker, someone who navigates insurance claims and takes intake calls. Throughout her story, she places her own interpretations of events above those of medically educated providers, therapists, and the families and patients that work with them. She claims to know better for these patients, and has acted to sabotage their care.
I have decided to do the work of going point by point through her entire story to show that all of this is indeed the case. Follow along:
Until 2015 or so, a very small number of these boys comprised the population of pediatric gender dysphoria cases. Then, across the Western world, there began to be a dramatic increase in a new population: Teenage girls, many with no previous history of gender distress, suddenly declared they were transgender and demanded immediate treatment with testosterone.
I certainly saw this at the center. One of my jobs was to do intake for new patients and their families. When I started there were probably 10 such calls a month. When I left there were 50, and about 70 percent of the new patients were girls. Sometimes clusters of girls arrived from the same high school.
Jamie starts right out of the gate with right wing talking points designed to paint transgender people as being a “trend” or “social contagion.” Her evidence for this claim is that her clinic saw an increase in transgender patients from 10 people to 50 people per month and that she saw more people assigned female at birth than assigned male at birth over that time period. The metropolitan population of St. Louis is 2.8 million people. If her clinic saw 1,000 people over 5 years, then she saw 0.03% of the local population that her clinic served. Given that we know up to 2% of Gen Z and younger identify as transgender, her clinic saw only a miniscule proportion of the transgender population – likely the ones that needed gender affirming care the most. This actually undercuts her argument of a massive social contagion when even most transgender youth did not seek nor receive care.
This section also alludes to ROGD, which says to me she has likely consumed a lot of anti-trans literature before writing it. The entire document is filled with evidence of such. The idea that Transgender people are “suddenly declaring their gender identity with no history” has also been flatly disputed by research. Instead, research has shown that trans youth know their identity for a long time before coming out, leading to some parents assuming that the onset of their gender dysphoria was “sudden” and “rapid.” Children often wait 3-6 or even more years before first declaring their gender identity and visiting a clinic.
Difference in the age of knowing gender identity and first visiting a clinic.
As for sex differences of coming out, this too has been disputed by research. Trans masculine individuals (who this writer references as “girls” and often misgenders throughout her document) are not “more likely” to identify as trans and social contagion is not an accurate description of transgender identification according to this research in the journal Pediatrics. Transgender boys have, in recent years, more easily found themselves able to come out and express themselves. Meanwhile, transgender girls, assigned male at birth, have been the target of anti-trans legislation banning them from sports, bathrooms, and more. If such differences do begin to manifest, especially in areas like St. Louis, there may be confounding local factors at play like excess targeting of transgender girls.
At any rate, Jamie Reed is not a researcher. She is not even a medical provider. She is a case worker that developed anti-trans opinions and has now engaged in activity that will harm this patient population. She has taken their trust and weaponized it against them in a sickening fashion.
The girls who came to us had many comorbidities: depression, anxiety, ADHD, eating disorders, obesity. Many were diagnosed with autism, or had autism-like symptoms. A report last year on a British pediatric transgender center found that about one-third of the patients referred there were on the autism spectrum.
Frequently, our patients declared they had disorders that no one believed they had. We had patients who said they had Tourette syndrome (but they didn’t); that they had tic disorders (but they didn’t); that they had multiple personalities (but they didn’t).
The doctors privately recognized these false self-diagnoses as a manifestation of social contagion. They even acknowledged that suicide has an element of social contagion. But when I said the clusters of girls streaming into our service looked as if their gender issues might be a manifestation of social contagion, the doctors said gender identity reflected something innate.
I’ve already covered social contagion, so I will move to her other points.
Here Jamie repeats anti-trans talking points here blaming gender dysphoria on all other things than being trans. Bizarrely, she includes obesity here. While many transgender people have concurrent disorders, there is no established research showing being “trans” is caused by anything else. Furthermore, research into autistic transgender individuals has stated that being prevented from transitioning due to an autism diagnosis could “cause increased levels of depression and anxiety.” The idea that autistic individuals cannot be LGBT+ unfairly targets autistic people who have pushed back hard against the idea that their diagnosis means they cannot experience genuine gender identities or seuxal orientations.
Furthermore, as a caseworker, Jamie is not evaluating these patients in depth. She is not the one sitting and listening to the patient talk about their mental health through a diagnostic lens, nor is she trained in that. She places her opinion on their diagnoses above the opinion of the patients doctors and therapists. This will be a common theme in her writing.
Lastly, concurrent mental health problems are often solved by transitioning. Things like depression and anxiety are often alleviated heavily. Studies have shown that gender affirming care reduces depression in 60% of transgender individuals and suicide attempts by up to 73% in trans youth. Many transgender people have reported that solving their dysphoria lead to increases in quality of life, and this is born out by the research.
Please support my independent reporting and activism on transgender legislation by subscribing. You help me keep this going and keep people informed.
To begin transitioning, the girls needed a letter of support from a therapist—usually one we recommended—who they had to see only once or twice for the green light. To make it more efficient for the therapists, we offered them a template for how to write a letter in support of transition. The next stop was a single visit to the endocrinologist for a testosterone prescription.
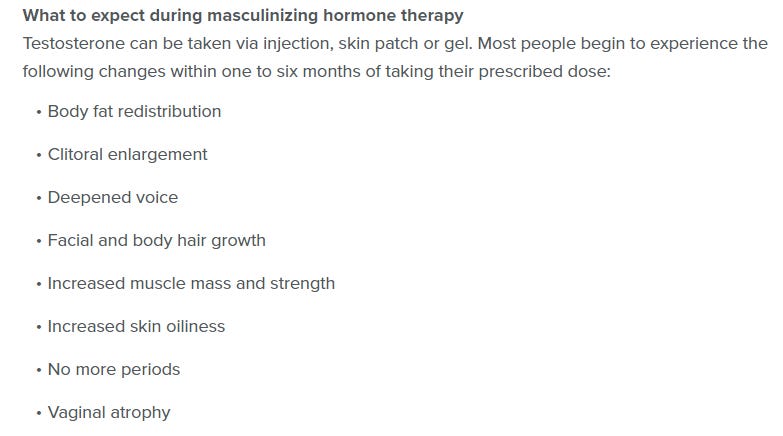
When a female takes testosterone, the profound and permanent effects of the hormone can be seen in a matter of months. Voices drop, beards sprout, body fat is redistributed. Sexual interest explodes, aggression increases, and mood can be unpredictable. Our patients were told about some side effects, including sterility. But after working at the center, I came to believe that teenagers are simply not capable of fully grasping what it means to make the decision to become infertile while still a minor.
There are several things to point out here. First of all, she admits that those who came through her clinic doors saw therapists. Secondly, though she says they only had to see the therapist once or twice, she does not state if that was the case for all or even most of her patients. It is indeed possible that most of her patients had continued to see therapists throughout their clinical journeys and beyond – this is certainly the case for most families of trans youth I have spoken to.
One thing that she points to as particularly damning is “template letters,” and this is something that any transgender person – trans adults included – are intimately familiar with. In order to get insurance coverage and approval, letters often have to follow very particular templates that touch on all aspects of what an insurance company looks for to provide care. In fact, many trans people have to switch therapists to someone who knows how to write these letters when they finally seek approval for gender affirming care. This is especially important to point out because Jamie leaves out of these people were obtaining psychological care before they arrived to her clinic, she states only that specific letters were written that required a couple of visits (likely by people trained in how to write letters properly). It is my own experience that transgender people, especially trans youth, often had plenty of therapy prior to engaging with a therapist who knew had to write a letter.
As for her other “effects,” these are all things that alleviate gender dysphoria in trans youth, resulting in the aforementioned 73% drop in suicide rates. I will not address them – these are intended effects of transition, albeit sensationalized, such as “unpredictable mood and aggression” which is pretty typical of teenage boy puberty.
Many encounters with patients emphasized to me how little these young people understood the profound impacts changing gender would have on their bodies and minds. But the center downplayed the negative consequences, and emphasized the need for transition. As the center’s website said, “Left untreated, gender dysphoria has any number of consequences, from self-harm to suicide. But when you take away the gender dysphoria by allowing a child to be who he or she is, we’re noticing that goes away. The studies we have show these kids often wind up functioning psychosocially as well as or better than their peers.”
There are no reliable studies showing this. Indeed, the experiences of many of the center’s patients prove how false these assertions are.
This is entirely true. Left untreated, gender dysphoria does result in self harm and suicide. Research has shown that gender affirming care results in a 73% reduction in suicide attempts. Another study showed a 40% drop with a sample size of 11,914 transgender youth. Other studies have shown similar results:
In fact, the findings around gender affirming care are so stunningly in favor of proceeding with that care that 29 major medical organizations representing hundreds of thousands of physicians have signed off to that care:
What does she use to contradict the 29 medical organizations and the scientific studies that show an improvement in suicide rates and mental health from gender affirming care?
A single article from Jesse Singal, an anti-trans writer who the LGBTQ+ rights organization GLAAD has described as having “built a career inaccurately writing about trans issues and targeting trans people.”
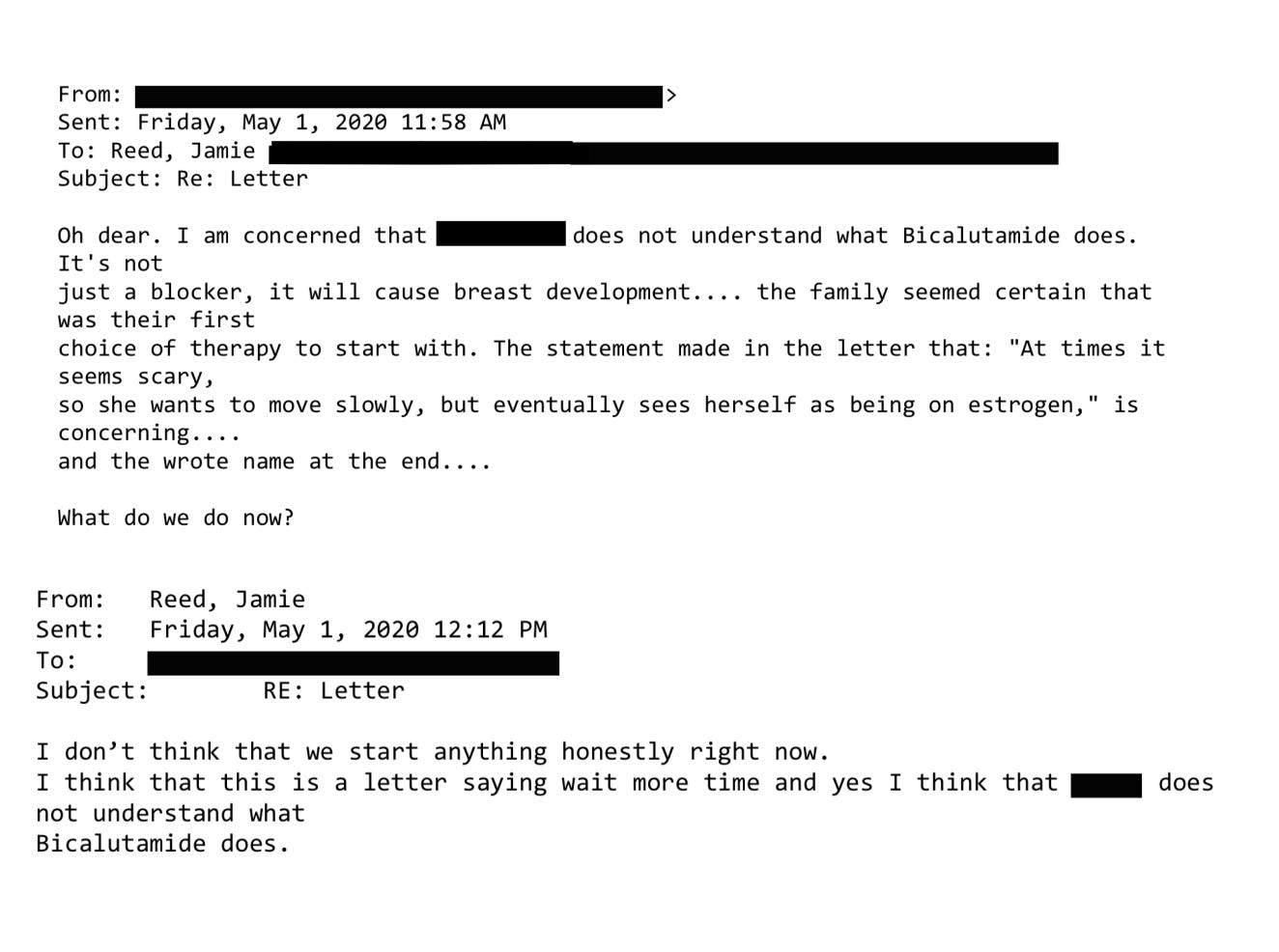
Here’s an example. On Friday, May 1, 2020, a colleague emailed me about a 15-year-old male patient: “Oh dear. I am concerned that [the patient] does not understand what Bicalutamide does.” I responded: “I don’t think that we start anything honestly right now.”
Interestingly, this letter actually shows that the clinic was taking precautions and undercuts the writer’s own point. They read what appears to be the psychological evaluation letters around a trans youth’s desire for treatment and determined that the bicalutamide was not the proper course of treatment for this transgender youth. Furthermore, reading the context clues around the letter where the transgender individual says “transition at times seems scary” is intimately familiar to any early-transition transgender person, especially a trans youth in a red state during years where transgender rights were being attacked more than ever.
Bicalutamide is a medication used to treat metastatic prostate cancer, and one of its side effects is that it feminizes the bodies of men who take it, including the appearance of breasts. The center prescribed this cancer drug as a puberty blocker and feminizing agent for boys. As with most cancer drugs, bicalutamide has a long list of side effects, and this patient experienced one of them: liver toxicity. He was sent to another unit of the hospital for evaluation and immediately taken off the drug. Afterward, his mother sent an electronic message to the Transgender Center saying that we were lucky her family was not the type to sue.
Anti-trans witnesses often try to use extremely explosive language to describe gender affirming care. Yes, Bicalutamide is used to treat “metastatic prostate cancer.” Bicalutamide is also used to treat hair loss and excessive facial hair in cisgender females. Furthermore, bicalutamide is not the first line treatment for most trans women but rather, spironolactone, a drug used to treat dozens of conditions including acne. That being said, rare side effects are possible with any drug including Tylenol, so the experience of a single patient having a bad experience with bicalutamide is not surprising and it appears that side effect was properly managed.
Please support my independent reporting and activism on transgender legislation by subscribing. You help me keep this going and keep people informed.
How little patients understood what they were getting into was illustrated by a call we received at the center in 2020 from a 17-year-old biological female patient who was on testosterone. She said she was bleeding from the vagina. In less than an hour she had soaked through an extra heavy pad, her jeans, and a towel she had wrapped around her waist. The nurse at the center told her to go to the emergency room right away.
We found out later this girl had had intercourse, and because testosterone thins the vaginal tissues, her vaginal canal had ripped open. She had to be sedated and given surgery to repair the damage. She wasn’t the only vaginal laceration case we heard about.
First I want to notice that, as the author has throughout her entire article, she misgenders the transgender boys who she is referring to. Not once does she refer to them with their proper pronouns. In this particular case, one patient experienced a very rare complication of a vaginal tear caused by hormone therapy combined with what appears to be vigorous sex. I want to highlight several things here:
She did not treat this patient and was not one of this patient’s providers.
There are well known protocols around vaginal care for trans men that include caring forvaginal walls.
Care compliance is an issue for all kinds of care that trans youth receive, not just gender affirming care.
Even with perfect care compliance, rare side effects can occur.
Remember that she has seen over a thousand patients, and she lists very few negative events. Though this claim is highly charged, she does not allege that the care itself was a net harm to this patient. It is very possible that this patient would not be alive without being provided gender affirming care. All of these costs and benefits as well as side effects are taken into account by her medical providers, not a desk worker with no experience in that direct care.
Other girls were disturbed by the effects of testosterone on their clitoris, which enlarges and grows into what looks like a microphallus, or a tiny penis. I counseled one patient whose enlarged clitoris now extended below her vulva, and it chafed and rubbed painfully in her jeans. I advised her to get the kind of compression undergarments worn by biological men who dress to pass as female. At the end of the call I thought to myself, “Wow, we hurt this kid.”
There are rare conditions in which babies are born with atypical genitalia—cases that call for sophisticated care and compassion. But clinics like the one where I worked are creating a whole cohort of kids with atypical genitals—and most of these teens haven’t even had sex yet. They had no idea who they were going to be as adults. Yet all it took for them to permanently transform themselves was one or two short conversations with a therapist.
This segment is flatly offensive to transgender people. Again, she misgenders the trans boys that she treats. She derides transgender genitals and discusses in negative terms things like an enlarged clitorus, which is something that many transgender men very much desire. Furthermore, this effect isvery plainly listed on the clinics own website and forms:
Lastly, she claims that these kids have no idea who they are going to be as adults, and yet trans kids do know their gender identities.97.5% of trans youth are stable in their gender identities even 5 years after social transition according to the journal Pediatrics.
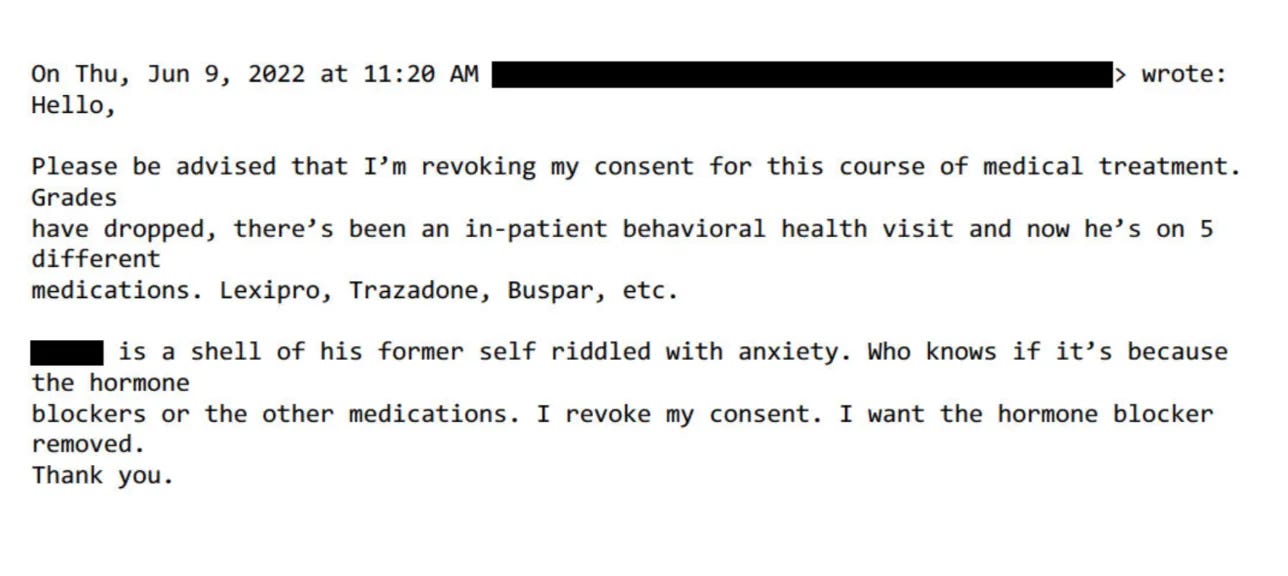
Being put on powerful doses of testosterone or estrogen—enough to try to trick your body into mimicking the opposite sex—-affects the rest of the body. I doubt that any parent who’s ever consented to give their kid testosterone (a lifelong treatment) knows that they’re also possibly signing their kid up for blood pressure medication, cholesterol medication, and perhaps sleep apnea and diabetes.
High blood pressure, high cholesterol, and sleep apnea are more common among men than women. This is not surprising or unusual. Gender affirming care changes the risk profile to the risk profile of the gender you have transitioned to.
But sometimes the parents’ understanding of what they had agreed to do to their children came forcefully:
This contradicts the idea that parents are having no input on their care. This parent withdrew consent, which can and does happen among trans youth. What we don’t know, however, is the health outcome of the kid whose consent was revoked. We are left to assume that things “improved” for this kid but sadly, we know that is not the case for most transgender youth.
Besides teenage girls, another new group was referred to us: young people from the inpatient psychiatric unit, or the emergency department, of St. Louis Children’s Hospital. The mental health of these kids was deeply concerning—there were diagnoses like schizophrenia, PTSD, bipolar disorder, and more. Often they were already on a fistful of pharmaceuticals.
This was tragic, but unsurprising given the profound trauma some had been through. Yet no matter how much suffering or pain a child had endured, or how little treatment and love they had received, our doctors viewed gender transition—even with all the expense and hardship it entailed—as the solution.
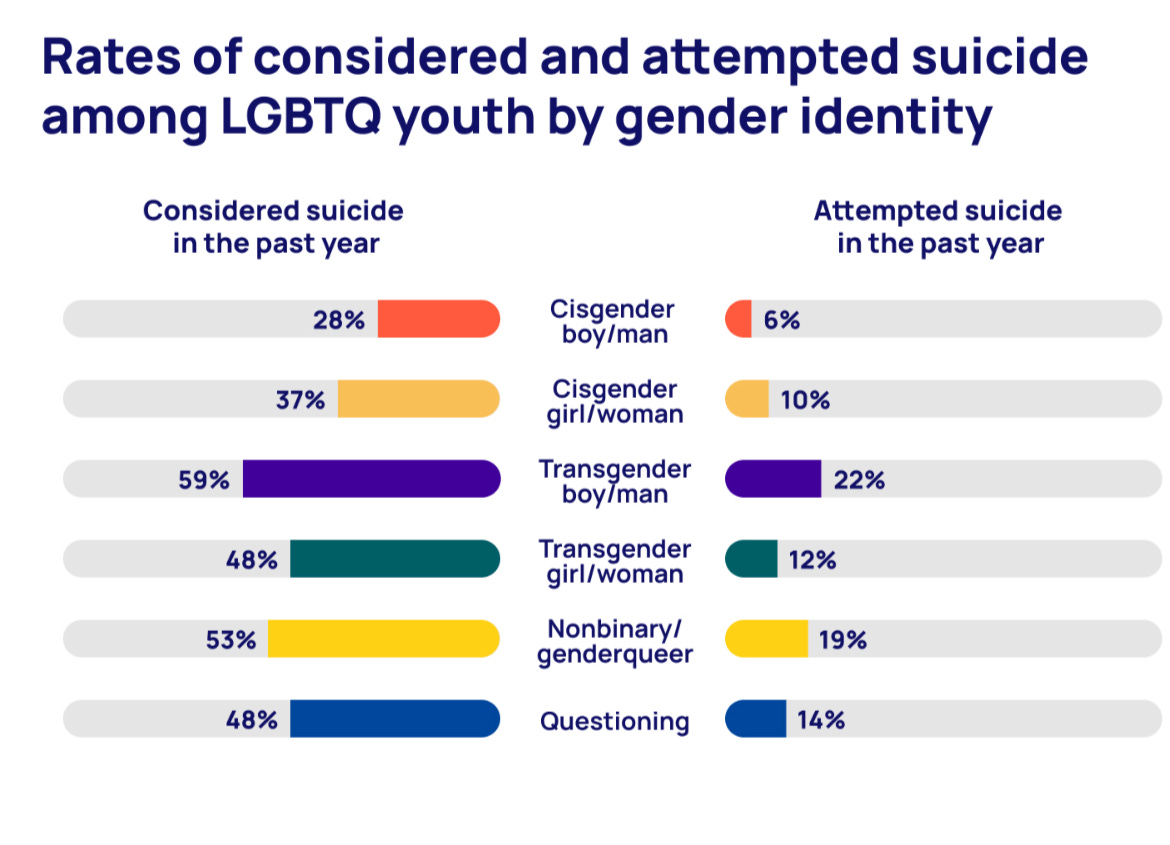
This portion is one of the saddest parts of Jamie’s anti-trans scree, because it shows the importance of gender affirming care and why it is so badly needed for so many trans youth. Often, a transgender person will not get help or medical care for their gender dysphoria until they attempt to take their own life. 40% of transgender people report having a suicide attempt. It is wholly unsurprising that Jamie’s first interaction with many trans youth is from inpatient psychiatrics units following severe mental health crises. Untreated gender dysphoria is deadly, and we know from aforementioned research that gender affirming care is the solution.
Furthermore, mental health among trans youth has been worsening due to laws targeting them,according to the Trevor Project.See this chart (more these are year over year rates):
Erin Reed @ErinInTheMorn
Legislators need to know the cruel impact that anti-trans bills have on trans people, who have statistically one of the highest suicide rates. Whenever anti trans bills are passed, suicide searches spike. When they are defeated, they go down. It’s that big a signal.
For example, one teenager came to us in the summer of 2022 when he was 17 years old and living in a lockdown facility because he had been sexually abusing dogs. He’d had an awful childhood: His mother was a drug addict, his father was imprisoned, and he grew up in foster care. Whatever treatment he may have been getting, it wasn’t working.
During our intake I learned from another caseworker that when he got out, he planned to reoffend because he believed the dogs had willingly submitted.
Somewhere along the way, he expressed a desire to become female, so he ended up being seen at our center. From there, he went to a psychologist at the hospital who was known to approve virtually everyone seeking transition. Then our doctor recommended feminizing hormones. At the time, I wondered if this was being done as a form of chemical castration.
She has seen over a thousand patients and is pointing to a single extreme shock story anecdote of someone who has experienced mental illness who came from an inpatient psychiatric unit. This person clearly has not “only seen one or two hours of therapy sessions” as some of the patients she alleges earlier. Instead, this trans youth has clearly gotten several evaluations from social workers, facility managers, and a psychologist. She did not assess this patient and was not involved in that, nor does she say how many assessments this patient received. She inserts her own opinion and her own interpretation of the situation here.
We also do not know what the result of this treatment was and if this person’s mental health saw improvements after treatment. Instead, we have her opinion that “this was done to chemically castrate this person.”
That same thought came up again with another case. This one was in spring of 2022 and concerned a young man who had intense obsessive-compulsive disorder that manifested as a desire to cut off his penis after he masturbated. This patient expressed no gender dysphoria, but he got hormones, too. I asked the doctor what protocol he was following, but I never got a straight answer.
As usual, she is misgendering this transgender patient. She claims that this patient expressed no gender dysphoria, but she does not claim to have personally assessed this patient. It is very possible that the patient was not forthcoming to her over the intake form, but was much more forthcoming to her doctors and therapists.
Another disturbing aspect of the center was its lack of regard for the rights of parents—and the extent to which doctors saw themselves as more informed decision-makers over the fate of these children.
In Missouri, only one parent’s consent is required for treatment of their child. But when there was a dispute between the parents, it seemed the center always took the side of the affirming parent.
She states that the center did not regard parents as having rights, and yet she points out that the clinic was directly following the law here. There is no allegation of wrongdoing here, only that she is upset that the center followed the law and allowed one parent to initiate medical care for their children based on best medical practices and guidelines. Missouri centers would likely not turn away a parent who was seeking care for their kid because they had experienced depression and needed an antidepressant either. If you follow the direction of all medical organizations and established research, the treatment of gender dysphoria does (and should) operate like other care in Missouri.
My concerns about this approach to dissenting parents grew in 2019 when one of our doctors actually testified in a custody hearing against a father who opposed a mother’s wish to start their 11-year-old daughter on puberty blockers.
I had done the original intake call, and I found the mother quite disturbing. She and the father were getting divorced, and the mother described the daughter as “kind of a tomboy.” So now the mother was convinced her child was trans. But when I asked if her daughter had adopted a boy’s name, if she was distressed about her body, if she was saying she felt like a boy, the mother said no. I explained the girl just didn’t meet the criteria for an evaluation.
Then a month later, the mother called back and said her daughter now used a boy’s name, was in distress over her body, and wanted to transition. This time the mom and daughter were given an appointment. Our providers decided the girl was trans and prescribed a puberty blocker to prevent her normal development.
This portion is extremely frustrating, because it seems that Jamie is upset that the doctors testified on a patient’s behalf that the best medical practices were followed. An entire court case happened around this proceeding where a judge weighed all of the evidence and statements and came to a verdict. We are supposed to put all of that aside because of a vendetta that Jamie has with her own place of employment.
I will highlight that in this case, she did not do the direct psychological assessment of the child. There are very simple reasons why she may have interpreted these events differently than how they actually occurred. For instance, on the initial intake, the parent may have not been given all of the information from the trans boy (again, she misgenders the patient). On the second visit, the parent may have provided more information that came as a result of the psychological assessment the boy gave.
This was likely explored in the court case, but Jamie wishes for you to take her interpretation of these events as true and wants to end care for an entire branch of patients because of that interpretation.
Because I was the main intake person, I had the broadest perspective on our existing and prospective patients. In 2019, a new group of people appeared on my radar: desisters and detransitioners. Desisters choose not to go through with a transition. Detransitioners are transgender people who decide to return to their birth gender.
The one colleague with whom I was able to share my concerns agreed with me that we should be tracking desistance and detransition. We thought the doctors would want to collect and understand this data in order to figure out what they had missed.
We were wrong. One doctor wondered aloud why he would spend time on someone who was no longer his patient.
Detransition is rare among trans youth – as mentioned before, it is only 2.5%. Interestingly, Jamie’s statements here do not allege any differently. Nowhere in her entire article does she state that there was an “explosion of detransitioners” or allege high numbers. This in a way confirms what we already know about the rarity of youth detransition.
One of the saddest cases of detransition I witnessed was a teenage girl, who, like so many of our patients, came from an unstable family, was in an uncertain living situation, and had a history of drug use. The overwhelming majority of our patients are white, but this girl was black. She was put on hormones at the center when she was around 16. When she was 18, she went in for a double mastectomy, what’s known as “top surgery.”
Three months later she called the surgeon’s office to say she was going back to her birth name and that her pronouns were “she” and “her.” Heartbreakingly, she told the nurse, “I want my breasts back.” The surgeon’s office contacted our office because they didn’t know what to say to this girl.
My colleague and I said that we would reach out. It took a while to track her down, and when we did we made sure that she was in decent mental health, that she was not actively suicidal, that she was not using substances. The last I heard, she was pregnant. Of course, she’ll never be able to breastfeed her child.
So instead of talking about high numbers of detransitioners or an “explosion” of them, like we often see alleged in anti-trans hearings, she instead focuses on single cases of detransitioners. This particular story is the only story of a detransitioner she can point to. I am sure she may have saw a handful of others, but given the dearth of detransitioners in her allegations, it would seem that her clinic was actually better at identifying youth who would be stable in their transition – otherwise she would be talking about how her clinic saw hundreds of detransitioners. Remember that anti-trans advocates claim that detransition rate is 85%, an easily disproven lie. See this tweet thread for my writing on this topic(click in and read the whole thread):
Erin Reed @ErinInTheMorn
Ever hear “80-90% of trans kids desist”? This is misleading and a lie. This comes from the DSM-4 criteria where any gender nonconforming kid was considered trans and counted under desistance. Likewise, trans kids COULD NOT transition and of course they “desisted.”
Here’s just one example: On January 6, 2022, I received an email from a staff therapist asking me for help with a case of a 16-year-old transgender male living in another state. “Parents are open to having patient see a therapist but are not supportive of gender and patient does not want parents to be aware of gender identity. I am having a challenging time finding a gender affirming therapist.”
I replied:
“I do not ethically agree with linking a minor patient to a therapist who would be gender affirming with gender as a focus of their work without that being discussed with the parents and the parent agreeing to that kind of care.”
All therapists who follow guidelines are “gender affirming.” This case manager, who is not a therapist herself, is advocating for trans youth to be sent to unaffirming therapists. In this particular case, the trans youth is concerned about not ending up in a conversion therapy situation – a very reasonable concern, especially with the advent of conversion therapy movements within the United Statestrying to target transgender people.
In all my years at the Washington University School of Medicine, I had received solidly positive performance reviews. But in 2021, that changed. I got a below-average mark for my “Judgment” and “Working Relationships/Cooperative Spirit.” Although I was described as “responsible, conscientious, hard-working and productive” the evaluation also noted: “At times Jamie responds poorly to direction from management with defensiveness and hostility.”
It sounds like she started getting negative reviews around the same time she started misgendering her patients and placing herself above the medical training of the doctors who work at the clinic as well as above the psychological training of their care teams.
Things came to a head at a half-day retreat in summer of 2022. In front of the team, the doctors said that my colleague and I had to stop questioning the “medicine and the science” as well as their authority. Then an administrator told us we had to “Get on board, or get out.” It became clear that the purpose of the retreat was to deliver these messages to us.
This is a good confrontation. As mentioned before, she is not a medical expert and does not do the in depth evaluation that the medical experts and psychological care teams do. Clearly she has a history of misgendering her trans patients. She saw herself as above best practices and medical guidelines. She elevates within her own mind the experience of edge case detransitioners and has given those with good results no credit and no voice.
The Washington University system provides a generous college tuition payment program for long-standing employees. I live by my paycheck and have no money to put aside for five college tuitions for my kids. I had to keep my job. I also feel a lot of loyalty to Washington University.
But I decided then and there that I had to get out of the Transgender Center, and to do so, I had to keep my head down and improve my next performance review.
I managed to get a decent evaluation, and I landed a job conducting research in another part of The Washington University School of Medicine. I gave my notice and left the Transgender Center in November of 2022.
Thank god she no longer cares for these patients.
For a couple of weeks, I tried to put everything behind me and settled into my new job as a clinical research coordinator, managing studies regarding children undergoing bone marrow transplants.
Then I came across comments from Dr. Rachel Levine, a transgender woman who is a high official at the federal Department of Health and Human Services. The article read: “Levine, the U.S. assistant secretary for health, said that clinics are proceeding carefully and that no American children are receiving drugs or hormones for gender dysphoria who shouldn’t.”
From her own letters, she shows that they were proceeding carefully and methodically. They identified cases of concern and the negative outcomes appear fairly rare given the over 1,000 patients she saw and the dearth of negative events. Furthermore, negative long term outcomes do not appear to be alleged in all but a couple patients out of the thousand patients she saw. Her own anecdotes do nothing to disprove this.
I felt stunned and sickened. It wasn’t true. And I know that from deep first-hand experience.
So I started writing down everything I could about my experience at the Transgender Center. Two weeks ago, I brought my concerns and documents to the attention of Missouri’s attorney general. He is a Republican. I am a progressive. But the safety of children should not be a matter for our culture wars.
Trans-exclusionary radical feminists often call themselves “liberal” or “progressive” but are anything but.
Given the secrecy and lack of rigorous standards that characterize youth gender transition across the country, I believe that to ensure the safety of American children, we need a moratorium on the hormonal and surgical treatment of young people with gender dysphoria.
I have already presented studies that show how many trans youth would take their lives if this happened. If she is truly concerned about her patient population, she would not advocate for this and against the medical science of dozens of the leading medical organizations.
In the past 15 years, according to Reuters, the U.S. has gone from having no pediatric gender clinics to more than 100. A thorough analysis should be undertaken to find out what has been done to their patients and why—and what the long-term consequences are.
Left handedness also exploded when left handed people were accommodated:
There is a clear path for us to follow. Just last year England announced that it would close the Tavistock’s youth gender clinic, then the NHS’s only such clinic in the country, after an investigation revealed shoddy practices and poor patient treatment. Sweden and Finland, too, have investigated pediatric transition and greatly curbed the practice, finding there is insufficient evidence of help, and danger of great harm.
It is so clear that she is working with the major anti-trans organizations in developing these calls to action. We have heard this in every Republican testimony for anti-trans bills this year. None of these countries have categorically banned gender affirming care for trans youth like she wants.
It is clear that anti-trans sources are using her testimony to attack gender affirming care nationwide for trans youth. I have no doubt that her story will be used to enact such bans in places like Tennessee, Texas, South Dakota, and Mississippi. Some of these bans will define gender affirming care as child abuse and take the kids of trans parents away. Let’s not gaslight ourselves into thinking that any of this is being done “for the good of children.” These policies have and will kill trans youth. Already, I have received four phone calls from the parents or friends of trans youth that have tried or completed attempts to take their own lives. That is the end goal of documents like this and anti-trans policies they add fuel to.
Please support my independent reporting and activism on transgender legislation by subscribing. You help me keep this going and keep people informed.
A balanced and well rounded report on rabid anti-trans Walsh getting called out at a hearing on creating laws on regulating trans kids healthcare. The hosts are fair in their reporting not giving a sensationalized view of the situation. But I give credit to the Tenn democrats that came armed with facts to shoot down Matt Walsh’s bigotry. If anyone wonders at the religion category for these anti trans videos is most anti-gay / trans stuff has roots in religious bigotry. Plus Welsh is a theocrat wanting to install religious rule in the US. Hugs
Florida Gov. Ron DeSantis has been featuring anti-vaxxer Dr. Jon Ward at COVID-19 events as he positions himself for a 2024 presidential run. Ward said in a podcast appearance last year that Dr. Anthony “Fauci should face a firing squad” because of his work.
Ward is a Florida dermatologist who, as Politico recently reported, has become “a central figure in DeSantis’ Covid-19 events.” He appeared at a COVID-19 press conference with DeSantis on January 17.
In August 2022, DeSantis appointed Ward to the Northwest Florida State College District Board of Trustees. Ward has linked the death of Lisa Marie Presley to “Pfizer and Moderna” and told parents to lie to schools about their children’s COVID-19 history.
Ward’s views are aligned with DeSantis’ on Covid. The Florida governor has built a national reputation by rejecting Covid-19 mandates such as masking students and vaccinating children. DeSantis’ surgeon general, Joe Ladapo, has also come under fire from the medical community for questioning vaccine safety and warning men against taking the Pfizer-BioNTech and Moderna Covid-19 vaccine.
Ward’s emergence as a central figure in DeSantis’ Covid-19 events has given rise to concern among many in Florida’s medical community, some members of which think Ward is, at best, misguided and, at worst, a dangerous font of misinformation. He also does not claim to be an expert on public health, a criticism frequently raised by critics who are concerned the governor is amplifying the views of a dermatologist without training in pandemic response.
Why not a proctologist… “Supposing we hit the body with a tremendous, whether it’s ultraviolet or just very powerful light,and then I said supposing you brought the light inside the body, which you can do either through the skin or in some other way.”
This is well known and the medical has repeatedly said that affirming the gender identity of the person while assisting with necessary age appropriate treatments including puberty blockers or hormone therapy when needed is the best medical practice. That is something the anti-trans people cannot refute, the majority of medical associations including the AMA and the largest pediatric medical associations believe in supporting trans people transitioning. But at the same time the red state republican leaders who mostly have no medical training are trying hard to ban or make the need medical assistance illegal. Why are they doing this? For political gain mostly, and religious indoctrination for others. This is very much like these same legislators denying abortion / reproductive rights to pregnant people or requiring women to cover their arms and where long skirts in state legislative bodies. It is people acting on an ideology to roll back advances in medical understanding and society to return to a time they feel more comfortable with. It is about their comfort not your needs and their ability to force their ignorance on others against the doctors best medical advice. ** BTW this happened to me in Florida. I was on a great medication for muscle spasms called Soma. The state legislators in an attempt to look tough on opioid addictions made it nearly impossible for pain doctors, and only pain doctors, to prescribe Soma. I spent months trying to get a replacement that worked and none were as good. **Hugs
Researchers tracked 315 trans and non-binary young people in what is reportedly the largest study in the U.S. to date.
Hormone therapy improves the mental health of transgender youth. That’s the takeaway from a new study from The New England Journal of Medicine, released last week.
The study is reportedly the largest in the U.S. to date. Over the course of two years, researchers tracked 315 trans and non-binary young people between the ages of 12 and 20 receiving hormone therapy. According to a summary of the research, “During the study period, appearance congruence (alignment between gender identity and physical appearance), positive affect, and life satisfaction increased, and depression and anxiety symptoms decreased.”
Researchers reported that young people who were assigned female at birth saw greater benefits when taking testosterone than those assigned male at birth who took estrogen. Several factors could be at play here, they speculated, including the speed with which the outward effects of testosterone manifest and greater social stigma faced by transfeminine people compared to transmasculine people.
The authors note that “marked increases in referrals but limited evidence as to long-term outcomes have led to controversies and debate” over providing adolescents with gender-affirming hormones (GAH). Across the U.S., state legislators have introduced bills restricting or outright banning gender-affirming care for transgender youth.
“Research like this is significant because it provides more longitudinal data,” Dr. Kareen Matouk, a clinical psychologist in the gender identity program at Columbia University Irving Medical Center, told Self magazine. “This helps individuals and their families navigate the health care system with more ease and confidence, and protects access to gender-affirming care that lawmakers are attempting to deny.”
Opponents of gender-affirming care for trans young people frequently argue that puberty blockers and GAH may have harmful or irreversible effects. But Matouk said, “We have some data suggesting that gender-affirming hormone therapy is generally safe and effective under the supervision of an endocrinologist or medical provider who specializes in transgender health care and has experience initiating hormone therapy.”
Gender-affirming care for both adolescents and adults has been endorsed by the American Medical Association, the American Academy of Pediatrics, the American Psychiatric Association, and many other professional groups as necessary and frequently lifesaving for transgender individuals.
While the authors of the new study stress that more research into other factors – including access to mental healthcare and the quality of peer relations and family support – is needed, their findings show that “that mental health improves with GAH, whereas withholding treatment may lead to increased gender dysphoria and adversely affect psychological functioning.”
Radical Right Republican Senator Rand Paul gave a speech before the Omnibus Spending Bill vote complaining about Government spending while misrepresenting examples. Meidas Contributor Texas Paul reacts in an epic takedown.
Quick update on me before the video that has information that everyone should hear. I hurt so bad right now I can only stand a few minutes before the pain is so bad I either have to sit or fall. Of course it is better earlier when I first get up by noon or 1 PM I can barely get up and go to the bathroom before the pain is so severe I am in danger of falling down. But if I sit the pain builds up in the upper part of my back instead of the lower part so again I have to move. Mostly right now it seems I get about 3 hours up at most and then 2 hours laying down. When I take enough medication to help cover the pain which lately has been the maximum of my medications, the next day I am sick to my stomach and have nausea issues. Think of it like being on a drunken night out at the bars, and how you would feel the next day. That lasts until I get enough medication back in my system again, and then if I take the maximum again I am sick the next day. It is a cycle I cannot stand. Be pain controlled in the afternoon and rest of the day while befuddled with confusion of the medications and the next morning wake up sick with a rolling stomach and nausea that either makes me vomit (three times yesterday) or just feel like I am going to vomit such as today when I did not vomit but felt I could until about 1 PM. I have an MRI on the 25th. I am losing the good from the last set of spine shots in the bottom of my spine, so tomorrow I need to call the pain clinic and see if they can adjust my appointment to get another set of spine epidurals for all three sections. Right now I am spending as much time laying down as I am upright. However this morning and yesterday morning Ron and I did take a short walk as we used to before the hurricane. It is much shorter than the other walks were because my back gives out and his hip starts to bother him too much to do a longer one. If the new spine shots don’t fix this, then I need to change medications to fentanyl or something as strong. The doctor tells me that fentanyl is much stronger than the medications I am currently taking. One last thing. Randy my wonderful brother has tried to get me to look at getting an over the bedside table like hospitals use and using a couple of the old laptops we have or at least the bedroom TV and a laptop to read and answer comments which I bitch constantly I am missing. Today Ron and I have started talking about it. It will depend on what the doctors can do. Hugs
Republicans cannot seem to care how their smoking hurts others around them who don’t smoke. Sad that in 2023 with all the information around about how bad tobacco both smoked or chewed is for both those that do it and those around them. But again republicans have a real issue trying to care about anyone other than themselves. Hugs
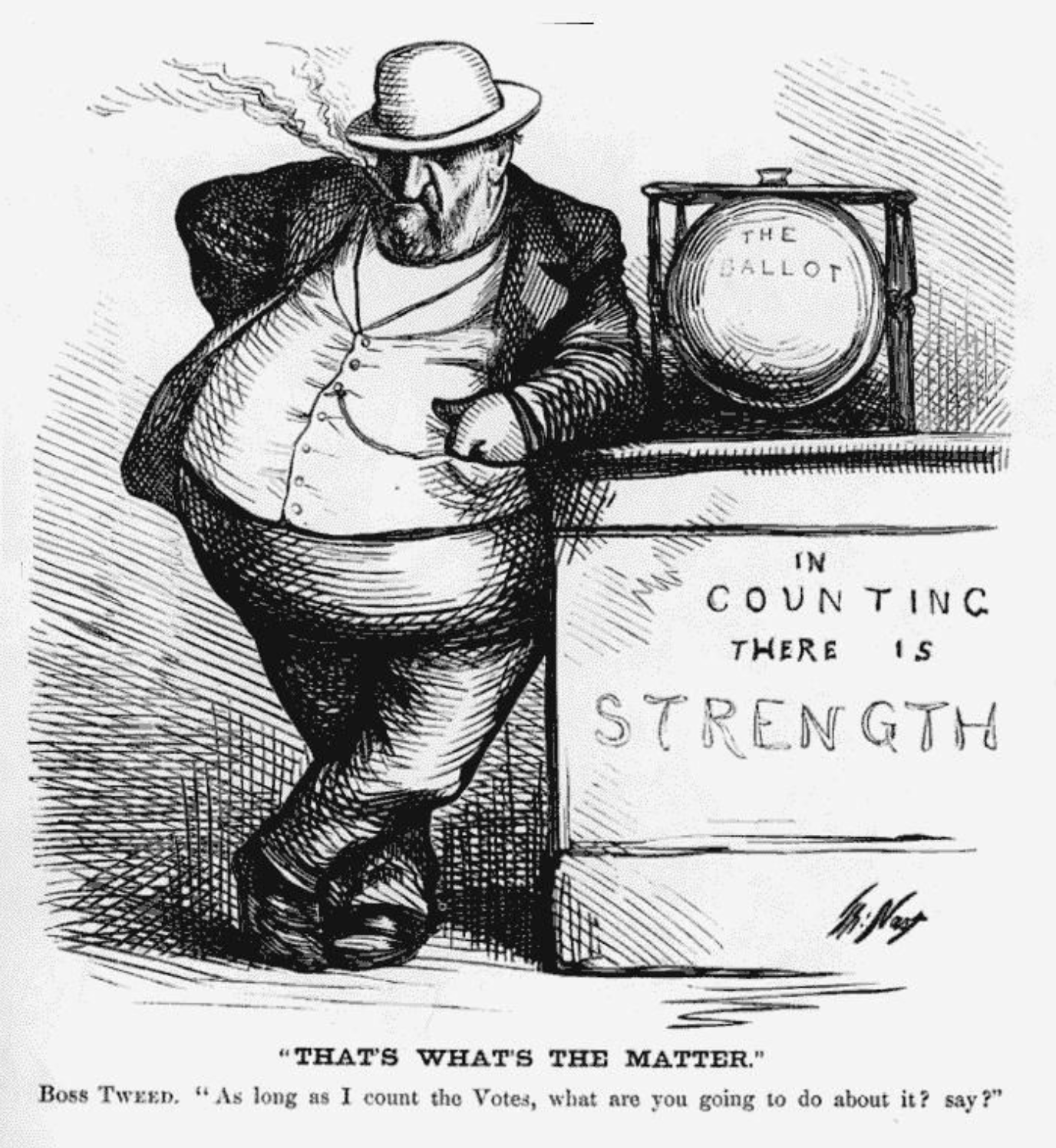
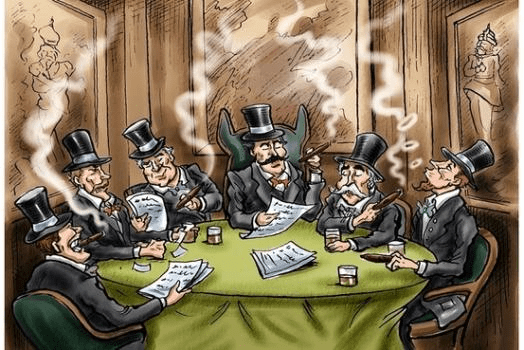
“Smoke ’em if you got ’em.” That’s not just the name of a 2004 Cypress Hill EP but also apparently the new rule in the GOP-controlled House. Republican members are lighting up their cigars in Congressional offices — and driving members of the press corps “insane in the brain” with the smell.
An executive order signed by President Bill Clinton in 1997 banned smoking in many federal buildings, but only those under the control of the Executive Branch. The laws in Washington, D.C. similarly ban smoking in indoor spaces, but again, that does not apply to congressional offices.
Yuck, cigarette and cigar smoke stinks. Inside buildings it spreads through the HVAC system and permeates everything, everyone’s clothing. It becomes in escapable. People who smoke reek of it; you can smell the stench when they walk into a room.
Republicans have been making life worse for everyone since 1968.
It literally does not apply to Congress – perhaps we need a constitutional amendment requiring members of Congress to be held to the same legal standards as other Americans – and perhaps their salaries should be tied to median incomes in their districts, and they should not have any better medical coverage or retirement benefits than ordinary Americans.
why don’t we totally go back to the 1950s – old white guys smoking cigars in the back offices making deals. how progressive. i’m surprised if they do not allow drinking on the House floor – it’ll be just like bowling!
The GOP oft reminisce about the “good old days” of the 50s…a white man’s world, where the US dominated the world economy, while much of the world was still recovering from WWII.
They do conveniently forget the 90% tax rate on the wealthy & corporations…which helped the middle class to grow & prosper.
It seems republicans are intent on exerting their right to be rude assholes no matter the cost to themselves or others. Please keep it up until you have turned public opinion solidly against your party.
The only thing the GOP think of pregnant staffers is “you’d better have that baby or you’ll be going to jail for murder. And don’t expect any handouts or time off”
When the new Resucklicans said they need to tear down the establishment, that’s the establishment they’re talking about: considering other’s welfare. They want to be obnoxious assholes again! Make me King of Assholes again! Trump is our Assholiness!
I would refuse to work in a smoke-filled office. Hopefully many of the junior staff will quit (or sue) rather than elect to get cancer form secondhand smoke. .
OT. Lawyer said we need to prosecute Donald Trump immediately. Sitting next to his Passport? Sounds like he’s going to turn them into big $$$fortune by selling us to Putin when he needs to escape justice to Putin his protector.
AND tfg had top secret docs literally sitting in the same drawer as his PASSPORT.
Gross. I’d be pissed if I was a staffer who had to go home every day with my clothes reeking of smoke. Dry cleaning ain’t free. That’s minuscule to the effects that kind of enclosed environment can have on people with asthma and other respiratory ailments.
Plus, that nasty, greasy residue will be settling all over inside the Capitol. I guess lathering the place with that residue isn’t too unexpected from the party that smeared their own feces around the building.
*shakes head* If Biden was really as awful as the Republicans say he is, they sure have some bizarre priorities now that they control the House.
I don’t care what people do with their own lives, and it gives me some comfort knowing these assholes are opening themselves up to an old age of sickness and likely a miserable death (both my parents died of smoking-related illnesses, not pretty) but I feel sorry for the reporters and staffers who are subjected to their secondhand smoke
My dogs that love gravy please make no mistake in thinking what these people are driving hard for. It is not the 1950s as most of us assume, but for these die hard Christian white male power nationalists the goal is the 1850s. Hugs
As of last week, Republican efforts to ban birth control in America have officially started, and teenagers in Texas are its first victims
To paraphrase Pastor Niemöller, first they came for our abortion rights. Now they’re coming for our birth control.
Psychologist Dr. Marty Klein notes at Psychology Today that there are typically only a few reasons why people oppose birth control. They are:
— Fundamentalist religions fear sexual pleasure, which birth control facilitates — Contraception effectively limits family size, empowering women — Contraception promotes personal autonomy [making women more likely to challenge male authority] — Birth control may make abortion more acceptable to society
As of last week, Republican efforts to ban birth control in America have officially started, and teenagers in Texas are its first victims.
When Clarence Thomas wrote in his Dobbs concurring opinion that the Supreme Court should next overturn the right to birth control in the United States, a lawyer and a judge in Texas were apparently listening.
Most Americans have no idea this high-stakes drama — heading toward the Supreme Court but already now law in Texas — is even going on.
Lost in the Christmas holiday chatter, a Trump-appointed federal district judge in Texas just a week ago put a stop to teenagers getting confidential access to federally-funded birth control pills and devices in that state.
He did it based on a lawsuit filed by attorney Jonathan Mitchell, the same man who co-authored the Texas “abortion vigilante” law. Everybody ridiculed that effort at first, you’ll recall, but the Supreme Court upheld it and today it’s Texas law and spreading across Red states like a fungus.
Mitchell is also known as the guy who supported the Mississippi abortion ban before the Supreme Court that led to the Dobbs decision overturning Roe v Wade.
Perhaps anticipating Clarence Thomas’ later call to overturn Supreme Court decisions legalizing birth control, homosexual behavior, and gay marriage (Griswold v Connecticut, Lawrence v Texas, Obergefell v Hodges), Mitchell even wrote in his amicus brief for the Dobbs case an originalist reference similar to the argument the Texas judge would later make against birth control:
“The right to marry an opposite-sex spouse is ‘deeply rooted in this Nation’s history and tradition’; the right to marry a same-sex spouse obviously is not.”
In the Texas federal lawsuit Mitchell brought, Deanda v. Becerra, Trump-appointed Judge Matthew Kacsmaryk ruled that teens between 15 and 18 shouldn’t be able to make birth control decisions independent of their parents because, he ruled, that had always been the law in the early years of America:
“For centuries, the common law held minors were incapable of giving consent to make important life decisions.”
Somehow, he managed to overlook the fact that the age of sexual consent “for centuries” was, in every American state from the founding of this nation in 1789, 10 to 12 years old. It wasn’t raised to 14, 15, or 16 in any US state until the 1930s.
But don’t try to argue facts with people running on religious or male-power arguments.
Although the fight for women’s bodily autonomy is as old as time, this part of the story begins in 1970.
Richard Nixon had a reputation as an awkward, bumbling prude when it came to sex, but even he knew that teenagers should be able to get birth control without their parents’ consent.
A teenage pregnancy could destroy a young woman’s life, and, at that time, over one-in-ten girls became pregnant between 15 and 19 years old. Fully 92 percent of those teenage pregnancies, according to research published in the following decade, were unintended and could have been prevented with access to birth control.
So, in 1970, President Nixon signed into law Title X, a federal grant program that included funds for confidential access to birth control for people across the nation regardless of their age.
Nonprofit agencies were formed in each state to receive the federal money and provide birth control (among other services): in Texas “Every Body Texas” is the group that administers Title X statewide through 32 agencies and 156 clinics.
The week of Christmas, because of Kacsmaryk’s Deanda v. Becerraruling, Texas agencies affiliated with Every Body Texas learned they had to start turning away teenagers, virtually all of them girls and women, who were seeking confidential birth control.
This is now the law in Texas.
Picking up the beat, Republican legislators in Missouri, Idaho, and Louisiana have introduced or are proposing birth control bans in those states, according to the Pew Trust. Expect Republicans in your state to soon try the same.
Lest you think that hyperbolic, consider how Republicans in the US House and Senate voted when Democrats introduced the Right to Contraception Actimmediatelyafter Clarence Thomas suggested the Court should overturn that right.
Fully 195 Republicans voted against the legislation in the House; only 8 supported it. And when it reached the Senate, it was killed by a Republican filibuster.
The Deanda v. Becerradecision in Texas banning confidential dispensing of contraception to teenagers will be appealed to the Fifth Circuit Court of Appeals, known across the nation as the place most likely to uphold crackpot rightwing rulings. From there it goes to the six crackpot rightwingers on the Supreme Court.
Republicans appear quite fixated on banning both abortion and birth control nationwide.
Authoritarian societies have a long history of trying to regulate women’s bodies.
The first books the Nazis burned in May of 1933 were birth control guides by Planned Parenthood founder Margaret Sanger, shortly before Hitler banned birth control in that nation (soldiers were allowed to possess condoms “to maintain their good health”).
Birth control was similarly banned in Romania by Nicolae Ceaușescu, bringing that nation Europe’s highest infant mortality rate and lowest life expectancy (particularly for women), a legacy which continues to this day even though Ceaușescu was overthrown and killed in 1989.
And now the GOP wants to ban birth control in the United States, starting with the youngest and most vulnerable among us. Authoritarians, after all, always first attack those least able to defend themselves before they climb the ladder of the society they intend to conquer.
This opening shot — coming out of Texas, just like the first ban on abortion (and from the same lawyer) — should make all Americans sit up and take notice.
Dr. Fauci humiliated Radical Right Wing Florida Governor Ron Desantis on Live TV a day after Desantis announced a grand jury to investigate COVID-19 Vaccine Manufacturers. Meidas Contributor Francis Maxwell reacts to this epic takedown.




 Legislators need to know the cruel impact that anti-trans bills have on trans people, who have statistically one of the highest suicide rates. Whenever anti trans bills are passed, suicide searches spike. When they are defeated, they go down. It’s that big a signal.
Legislators need to know the cruel impact that anti-trans bills have on trans people, who have statistically one of the highest suicide rates. Whenever anti trans bills are passed, suicide searches spike. When they are defeated, they go down. It’s that big a signal.