In 1 minute, a senate committee in Kansas will be holding a hearing to ban gender affirming care up to the age of 21.
It is one of the most cruel anti-trans bans in the country.
I will be covering it live. Follow along.
🧵
As always, I rely on people like you to do my work. Please consider subscribing to support me at my newsletter, where you'll get over 200 articles focusing on trans news around legislation and life moving across the United States per year.
"I have to remove my hair with laser hair removal"
(advocates for a bill that will force hundreds of trans amab youth through a male puberty which will result in them having to go through laser hair removal and expensive surgeries as adults)
This guy is testifying from "Mass Resistance."
This organization is responsible for a book called "The Hazards of Homosexuality," a pro-conversion therapy outlet that calls gay people's existance a "public health issue"
Dr. Gaylyn Perry is speaking not on behalf of any medical organization.
She’s a pulmonologist, not an endocrinologist.
She’s a sleep therapist.
Also she's stating that Europe is "closing its clinics."
Not a single country she is referring to has categorically banned gender affirming care.
From the Alabama lawsuit, relying on Europe helped sink that bill in court:
"No country in Europe has categorically banned gender affirming care"
Now a retired doctor is testifying.
“I’m here to speak the truth about natural law and the truth given to us by our savior.”
This is not medically oriented testimony and his belief in god should have no bearing on the right of parents to make decisions for their kids.
This doctor is using the old 2011 study of "19x suicide rates" among trans people.
This is an inaccurate reading of the Dhejne study, who has specifically come out against people reading it that way:
Essentially, they are comparing a specific high risk group trans people to the general public, and not to trans people with no interventions, and it was also looking at a 30 year retrospective during some of the worst acceptance of trans people in history. (1980s)
A representative of the Kansas American Academy of Pediatrics with 450 physicians in Kansas.
She’s saying that this decision should be between doctors and patients and families.
The ACLU of KS representative is speaking.
"This bill violates the constitutional rights of children, parents, and doctors"
“It places politicians feelings against medical advice of hundreds of thousands of doctors”
"Every state attempting to defend these bills has lost"
“People will die. Families will suffer. The practice of medicine will be compromised.”
“The very care this bill attacks is responsible for my life.”
Another trans person, a trans man, is speaking.
He was on puberty blockers til 17, and took testosterone.
“College was much easier after I had my medical interventions to be my true self.”
“I can’t imagine such a life without them.”
A WPATH Doctor is speaking.
“This bill will directly impact the lives of transgender youth, directly impacting lives. Their blood will be on your hands. This is unethical.”
"For a minor to access gender affirming care, I ensure in collaboration with mental health experts assess the consistent, insistent, and persistent presence of gender dysphoria and require consent from parents" and she talks about all of the hoops patients have to jump through.
Reverend Kayla Simons Wood is speaking on behalf of Kansas Interaction.
Submits testimony from 10 clergy opposing this bill.
“I and many other Christians believe trans people are created in Gods image.”
Beth Oller:
“I provide full spectrum care from babies to end of life and I provide gender affirming care. I am an actual practicing Kansas physician.”
“The majority of people detransition not because they are not trans, but because of violence and difficulties with family”
"We need to listen to their perspective rather than the curated presentation in front of you"
Senator Stephen is asking Dr. Hubbard, a WPATH doctor, a question.
"Ms. Hubbard, Are you telling me the AAP unwaiveringly supports surgical interventions"
Dr. Hubbard: “I would appreciate it if you refer to me as Dr. Hubbard, please.”
Then points out that the treatments are tailored to the individuals.
Questioner: "Can you tell me where from Kansas you received your gender affirming care?"
"I'm not from Kansas…"
Questioner: "Is this the first time you've testified?"
"No…"
Asking Dr Crabs:
"Your testimony was from the 1980s about transgender suicides. So not current. Can I ask you where you practiced?"
"I did not practice here"
"can you verify you had a license in kansas?"
The chair cut her off.
Now a Senator is asking Dr. Beth Oller where she works (one of the people against the bill):
The doctor responds she works in Kansas.
Strongly pointing out that all of the people in support of the bill are coming from out of state.
Now a Senator is asking one of the trans man transitioners if he was given all of the info around his transition.
He answers in the affirmative.
Now they are asking a question of one of the detransitioners,
"Do you believe you were groomed into the decision to transition?"
“I don’t believe in using that word… it’s too divisive…”
This hearing isn't going super well for them.
(They'll probably still vote it through)
ACLU witness:
“I am referring to the 1.3 million doctors that are represented by the medical organizations that support this care.”
This Senator is claiming puberty blockers and HRT are causing early onset cancer.
There’s no evidence of any sort of outbreak of early onset cancer in trans youth.
Asked of the AAP representative if the majority supports gender affirming care in their chapter.
She testifies yes, most of the 450 do.
Now she is asking about the Missouri whistleblower.
“A radical supporter of the far left has blown the whistle”
“Are there other areas of medical practice where the child directs their health care?”
The doctor: “Everything the child is involved in, but the child themselves does not direct gender diverse issues. It’s parents, doctors”
The doctor in the zoom call wanted to jump in and answer, but the chair cut the committee short and immediately adjourned.
I guess we're done for the day?
That was abrupt.
I have never seen such a rushed hearing with so few witnesses called forward… what the heck did I just see?
Sorry to those of you who showed up to testify who didn't get to.
Well… thanks for following along. We'll watch to see how they vote. Please support my independent reporting and activism by subscribing.
It did not take long for the facts to come out and totally debunk the latest anti-trans conspiracy TERF talking point but sadly the planned damage was already underway. This woman who worked at a clinic claims she sees kids forced to transition and gives a screed that reinforced every right-wing talking point, which have been proven wrong time and time again by medical and demographic studies. Turns out this exposé was of course a fake bunch of lies by an anti-trans person trying to sabotage medical care for trans kids during the legislative session. If you want the facts, read the article. Hugs
I have spend most of my day on this. My morning was spend helping a confused elderly couple with their clogged printer head because they have not printed in years and now want to do so. I got it to start working by repeatedly doing the head clean, yet they did not even know where they paper went in the machine. They were laying it on top, wonder it worked at all. So after I came home and ate, I took my medications and came down with a very severe allergic reaction that is only now trying to abate. As any long time follower will know I have life threatening allergies and even though I felt I could handle it due to the entire body response including the genital area Ron lost his composure demanding I take more Benadryl than I had and thought I should to stop the cascade of reaction. But regardless as the extra Benadryl would only make me more tired and sleepy, I gave in. Must keep peace in the home / family. So I am very tired, irritable, hurting, and have to go back tomorrow morning to help the couple I was helping today as they screwed everything up. So I will leave comments open and try to monitor them. If they go from facts and feelings to fringe stuff, conspiracies, and already debunked myths that are countered by the best practices approved by the majority of medical communities then I will shut them off. Best wishes. Hugs
Jamie Reed’s story is being pushed by the worst of the worst anti-trans voices on the internet. I dig point-by-point through her claims and show how they undermine her conclusions.
Please support my independent reporting and activism on transgender legislation by subscribing. You help me keep this going and keep people informed.
On February 9th, a former case worker at the Washington University’s Transgender Center at St. Louis Children’s Hospital released an article in The Free Press alleging widespread wrongdoing among clinicians in treating transgender patients. Within hours, right wing sources across the internet were carrying her story. Anti-trans organization Genspect, which has advocated for bans on gender affirming care up to the age of 25 years old, announced an interview with her live. The Republican attorney general of Missouri announced an investigation. Vernadette Broyles, an attorney who has tried several cases to overturn transgender policies in schools and who advised Ron DeSantis on the Don’t Say Gay law, was tapped to represent her. This has all of the markings of a manufactured controversy similar to Project Veritas’ Planned Parenthood Fetal Tissue, and similar groups are lining up behind this story.
We know that this story has been held back for at least two weeks and judging from the timing of the anti-trans bills heard in Missouri, the speed in which right wing outlets carried the story, and its release in the middle of the legislative season with the most attacks on transgender rights and healthcare in history, it’s hard not to see this as entirely planned. Delving into Jamie Reed’s allegations and story makes it clear that she is not an ideologically neutral individual on the care and respect of transgender people. Her statements and omissions reveal a clear ideological bias, and the organizations and representation she has chosen to work with contradict her claim that she “supports transgender people.”
Throughout her story, she frequently misgenders her patients. In fact, I am not aware of a single case where she genders her trans patients correctly. Out of the thousand or so patients she has seen, she only references a half dozen specific anecdotes of what she relays as poor experiences for transgender youth patients – anecdotes I will cover in detail. Even in these anecdotes, she often omits long term net harm. She leaves out the stories of what must be the rest of the thousand patients who, as we have seen in numerous testimony in hearings this year, saw their mental and physical health improve dramatically. Ultimately, she calls for stopping gender affirming care for trans youth – something that would result in actual harm and death to this patient population.
She is not a doctor, a psychologist, a psychiatrist, and does not have direct medical diagnostic experience with patients. She is a case worker, someone who navigates insurance claims and takes intake calls. Throughout her story, she places her own interpretations of events above those of medically educated providers, therapists, and the families and patients that work with them. She claims to know better for these patients, and has acted to sabotage their care.
I have decided to do the work of going point by point through her entire story to show that all of this is indeed the case. Follow along:
Until 2015 or so, a very small number of these boys comprised the population of pediatric gender dysphoria cases. Then, across the Western world, there began to be a dramatic increase in a new population: Teenage girls, many with no previous history of gender distress, suddenly declared they were transgender and demanded immediate treatment with testosterone.
I certainly saw this at the center. One of my jobs was to do intake for new patients and their families. When I started there were probably 10 such calls a month. When I left there were 50, and about 70 percent of the new patients were girls. Sometimes clusters of girls arrived from the same high school.
Jamie starts right out of the gate with right wing talking points designed to paint transgender people as being a “trend” or “social contagion.” Her evidence for this claim is that her clinic saw an increase in transgender patients from 10 people to 50 people per month and that she saw more people assigned female at birth than assigned male at birth over that time period. The metropolitan population of St. Louis is 2.8 million people. If her clinic saw 1,000 people over 5 years, then she saw 0.03% of the local population that her clinic served. Given that we know up to 2% of Gen Z and younger identify as transgender, her clinic saw only a miniscule proportion of the transgender population – likely the ones that needed gender affirming care the most. This actually undercuts her argument of a massive social contagion when even most transgender youth did not seek nor receive care.
This section also alludes to ROGD, which says to me she has likely consumed a lot of anti-trans literature before writing it. The entire document is filled with evidence of such. The idea that Transgender people are “suddenly declaring their gender identity with no history” has also been flatly disputed by research. Instead, research has shown that trans youth know their identity for a long time before coming out, leading to some parents assuming that the onset of their gender dysphoria was “sudden” and “rapid.” Children often wait 3-6 or even more years before first declaring their gender identity and visiting a clinic.
Difference in the age of knowing gender identity and first visiting a clinic.
As for sex differences of coming out, this too has been disputed by research. Trans masculine individuals (who this writer references as “girls” and often misgenders throughout her document) are not “more likely” to identify as trans and social contagion is not an accurate description of transgender identification according to this research in the journal Pediatrics. Transgender boys have, in recent years, more easily found themselves able to come out and express themselves. Meanwhile, transgender girls, assigned male at birth, have been the target of anti-trans legislation banning them from sports, bathrooms, and more. If such differences do begin to manifest, especially in areas like St. Louis, there may be confounding local factors at play like excess targeting of transgender girls.
At any rate, Jamie Reed is not a researcher. She is not even a medical provider. She is a case worker that developed anti-trans opinions and has now engaged in activity that will harm this patient population. She has taken their trust and weaponized it against them in a sickening fashion.
The girls who came to us had many comorbidities: depression, anxiety, ADHD, eating disorders, obesity. Many were diagnosed with autism, or had autism-like symptoms. A report last year on a British pediatric transgender center found that about one-third of the patients referred there were on the autism spectrum.
Frequently, our patients declared they had disorders that no one believed they had. We had patients who said they had Tourette syndrome (but they didn’t); that they had tic disorders (but they didn’t); that they had multiple personalities (but they didn’t).
The doctors privately recognized these false self-diagnoses as a manifestation of social contagion. They even acknowledged that suicide has an element of social contagion. But when I said the clusters of girls streaming into our service looked as if their gender issues might be a manifestation of social contagion, the doctors said gender identity reflected something innate.
I’ve already covered social contagion, so I will move to her other points.
Here Jamie repeats anti-trans talking points here blaming gender dysphoria on all other things than being trans. Bizarrely, she includes obesity here. While many transgender people have concurrent disorders, there is no established research showing being “trans” is caused by anything else. Furthermore, research into autistic transgender individuals has stated that being prevented from transitioning due to an autism diagnosis could “cause increased levels of depression and anxiety.” The idea that autistic individuals cannot be LGBT+ unfairly targets autistic people who have pushed back hard against the idea that their diagnosis means they cannot experience genuine gender identities or seuxal orientations.
Furthermore, as a caseworker, Jamie is not evaluating these patients in depth. She is not the one sitting and listening to the patient talk about their mental health through a diagnostic lens, nor is she trained in that. She places her opinion on their diagnoses above the opinion of the patients doctors and therapists. This will be a common theme in her writing.
Lastly, concurrent mental health problems are often solved by transitioning. Things like depression and anxiety are often alleviated heavily. Studies have shown that gender affirming care reduces depression in 60% of transgender individuals and suicide attempts by up to 73% in trans youth. Many transgender people have reported that solving their dysphoria lead to increases in quality of life, and this is born out by the research.
Please support my independent reporting and activism on transgender legislation by subscribing. You help me keep this going and keep people informed.
To begin transitioning, the girls needed a letter of support from a therapist—usually one we recommended—who they had to see only once or twice for the green light. To make it more efficient for the therapists, we offered them a template for how to write a letter in support of transition. The next stop was a single visit to the endocrinologist for a testosterone prescription.
When a female takes testosterone, the profound and permanent effects of the hormone can be seen in a matter of months. Voices drop, beards sprout, body fat is redistributed. Sexual interest explodes, aggression increases, and mood can be unpredictable. Our patients were told about some side effects, including sterility. But after working at the center, I came to believe that teenagers are simply not capable of fully grasping what it means to make the decision to become infertile while still a minor.
There are several things to point out here. First of all, she admits that those who came through her clinic doors saw therapists. Secondly, though she says they only had to see the therapist once or twice, she does not state if that was the case for all or even most of her patients. It is indeed possible that most of her patients had continued to see therapists throughout their clinical journeys and beyond – this is certainly the case for most families of trans youth I have spoken to.
One thing that she points to as particularly damning is “template letters,” and this is something that any transgender person – trans adults included – are intimately familiar with. In order to get insurance coverage and approval, letters often have to follow very particular templates that touch on all aspects of what an insurance company looks for to provide care. In fact, many trans people have to switch therapists to someone who knows how to write these letters when they finally seek approval for gender affirming care. This is especially important to point out because Jamie leaves out of these people were obtaining psychological care before they arrived to her clinic, she states only that specific letters were written that required a couple of visits (likely by people trained in how to write letters properly). It is my own experience that transgender people, especially trans youth, often had plenty of therapy prior to engaging with a therapist who knew had to write a letter.
As for her other “effects,” these are all things that alleviate gender dysphoria in trans youth, resulting in the aforementioned 73% drop in suicide rates. I will not address them – these are intended effects of transition, albeit sensationalized, such as “unpredictable mood and aggression” which is pretty typical of teenage boy puberty.
Many encounters with patients emphasized to me how little these young people understood the profound impacts changing gender would have on their bodies and minds. But the center downplayed the negative consequences, and emphasized the need for transition. As the center’s website said, “Left untreated, gender dysphoria has any number of consequences, from self-harm to suicide. But when you take away the gender dysphoria by allowing a child to be who he or she is, we’re noticing that goes away. The studies we have show these kids often wind up functioning psychosocially as well as or better than their peers.”
There are no reliable studies showing this. Indeed, the experiences of many of the center’s patients prove how false these assertions are.
This is entirely true. Left untreated, gender dysphoria does result in self harm and suicide. Research has shown that gender affirming care results in a 73% reduction in suicide attempts. Another study showed a 40% drop with a sample size of 11,914 transgender youth. Other studies have shown similar results:
In fact, the findings around gender affirming care are so stunningly in favor of proceeding with that care that 29 major medical organizations representing hundreds of thousands of physicians have signed off to that care:
What does she use to contradict the 29 medical organizations and the scientific studies that show an improvement in suicide rates and mental health from gender affirming care?
A single article from Jesse Singal, an anti-trans writer who the LGBTQ+ rights organization GLAAD has described as having “built a career inaccurately writing about trans issues and targeting trans people.”
Here’s an example. On Friday, May 1, 2020, a colleague emailed me about a 15-year-old male patient: “Oh dear. I am concerned that [the patient] does not understand what Bicalutamide does.” I responded: “I don’t think that we start anything honestly right now.”
Interestingly, this letter actually shows that the clinic was taking precautions and undercuts the writer’s own point. They read what appears to be the psychological evaluation letters around a trans youth’s desire for treatment and determined that the bicalutamide was not the proper course of treatment for this transgender youth. Furthermore, reading the context clues around the letter where the transgender individual says “transition at times seems scary” is intimately familiar to any early-transition transgender person, especially a trans youth in a red state during years where transgender rights were being attacked more than ever.
Bicalutamide is a medication used to treat metastatic prostate cancer, and one of its side effects is that it feminizes the bodies of men who take it, including the appearance of breasts. The center prescribed this cancer drug as a puberty blocker and feminizing agent for boys. As with most cancer drugs, bicalutamide has a long list of side effects, and this patient experienced one of them: liver toxicity. He was sent to another unit of the hospital for evaluation and immediately taken off the drug. Afterward, his mother sent an electronic message to the Transgender Center saying that we were lucky her family was not the type to sue.
Anti-trans witnesses often try to use extremely explosive language to describe gender affirming care. Yes, Bicalutamide is used to treat “metastatic prostate cancer.” Bicalutamide is also used to treat hair loss and excessive facial hair in cisgender females. Furthermore, bicalutamide is not the first line treatment for most trans women but rather, spironolactone, a drug used to treat dozens of conditions including acne. That being said, rare side effects are possible with any drug including Tylenol, so the experience of a single patient having a bad experience with bicalutamide is not surprising and it appears that side effect was properly managed.
Please support my independent reporting and activism on transgender legislation by subscribing. You help me keep this going and keep people informed.
How little patients understood what they were getting into was illustrated by a call we received at the center in 2020 from a 17-year-old biological female patient who was on testosterone. She said she was bleeding from the vagina. In less than an hour she had soaked through an extra heavy pad, her jeans, and a towel she had wrapped around her waist. The nurse at the center told her to go to the emergency room right away.
We found out later this girl had had intercourse, and because testosterone thins the vaginal tissues, her vaginal canal had ripped open. She had to be sedated and given surgery to repair the damage. She wasn’t the only vaginal laceration case we heard about.
First I want to notice that, as the author has throughout her entire article, she misgenders the transgender boys who she is referring to. Not once does she refer to them with their proper pronouns. In this particular case, one patient experienced a very rare complication of a vaginal tear caused by hormone therapy combined with what appears to be vigorous sex. I want to highlight several things here:
She did not treat this patient and was not one of this patient’s providers.
There are well known protocols around vaginal care for trans men that include caring forvaginal walls.
Care compliance is an issue for all kinds of care that trans youth receive, not just gender affirming care.
Even with perfect care compliance, rare side effects can occur.
Remember that she has seen over a thousand patients, and she lists very few negative events. Though this claim is highly charged, she does not allege that the care itself was a net harm to this patient. It is very possible that this patient would not be alive without being provided gender affirming care. All of these costs and benefits as well as side effects are taken into account by her medical providers, not a desk worker with no experience in that direct care.
Other girls were disturbed by the effects of testosterone on their clitoris, which enlarges and grows into what looks like a microphallus, or a tiny penis. I counseled one patient whose enlarged clitoris now extended below her vulva, and it chafed and rubbed painfully in her jeans. I advised her to get the kind of compression undergarments worn by biological men who dress to pass as female. At the end of the call I thought to myself, “Wow, we hurt this kid.”
There are rare conditions in which babies are born with atypical genitalia—cases that call for sophisticated care and compassion. But clinics like the one where I worked are creating a whole cohort of kids with atypical genitals—and most of these teens haven’t even had sex yet. They had no idea who they were going to be as adults. Yet all it took for them to permanently transform themselves was one or two short conversations with a therapist.
This segment is flatly offensive to transgender people. Again, she misgenders the trans boys that she treats. She derides transgender genitals and discusses in negative terms things like an enlarged clitorus, which is something that many transgender men very much desire. Furthermore, this effect isvery plainly listed on the clinics own website and forms:
Lastly, she claims that these kids have no idea who they are going to be as adults, and yet trans kids do know their gender identities.97.5% of trans youth are stable in their gender identities even 5 years after social transition according to the journal Pediatrics.
Being put on powerful doses of testosterone or estrogen—enough to try to trick your body into mimicking the opposite sex—-affects the rest of the body. I doubt that any parent who’s ever consented to give their kid testosterone (a lifelong treatment) knows that they’re also possibly signing their kid up for blood pressure medication, cholesterol medication, and perhaps sleep apnea and diabetes.
High blood pressure, high cholesterol, and sleep apnea are more common among men than women. This is not surprising or unusual. Gender affirming care changes the risk profile to the risk profile of the gender you have transitioned to.
But sometimes the parents’ understanding of what they had agreed to do to their children came forcefully:
This contradicts the idea that parents are having no input on their care. This parent withdrew consent, which can and does happen among trans youth. What we don’t know, however, is the health outcome of the kid whose consent was revoked. We are left to assume that things “improved” for this kid but sadly, we know that is not the case for most transgender youth.
Besides teenage girls, another new group was referred to us: young people from the inpatient psychiatric unit, or the emergency department, of St. Louis Children’s Hospital. The mental health of these kids was deeply concerning—there were diagnoses like schizophrenia, PTSD, bipolar disorder, and more. Often they were already on a fistful of pharmaceuticals.
This was tragic, but unsurprising given the profound trauma some had been through. Yet no matter how much suffering or pain a child had endured, or how little treatment and love they had received, our doctors viewed gender transition—even with all the expense and hardship it entailed—as the solution.
This portion is one of the saddest parts of Jamie’s anti-trans scree, because it shows the importance of gender affirming care and why it is so badly needed for so many trans youth. Often, a transgender person will not get help or medical care for their gender dysphoria until they attempt to take their own life. 40% of transgender people report having a suicide attempt. It is wholly unsurprising that Jamie’s first interaction with many trans youth is from inpatient psychiatrics units following severe mental health crises. Untreated gender dysphoria is deadly, and we know from aforementioned research that gender affirming care is the solution.
Furthermore, mental health among trans youth has been worsening due to laws targeting them,according to the Trevor Project.See this chart (more these are year over year rates):
Erin Reed @ErinInTheMorn
Legislators need to know the cruel impact that anti-trans bills have on trans people, who have statistically one of the highest suicide rates. Whenever anti trans bills are passed, suicide searches spike. When they are defeated, they go down. It’s that big a signal.
For example, one teenager came to us in the summer of 2022 when he was 17 years old and living in a lockdown facility because he had been sexually abusing dogs. He’d had an awful childhood: His mother was a drug addict, his father was imprisoned, and he grew up in foster care. Whatever treatment he may have been getting, it wasn’t working.
During our intake I learned from another caseworker that when he got out, he planned to reoffend because he believed the dogs had willingly submitted.
Somewhere along the way, he expressed a desire to become female, so he ended up being seen at our center. From there, he went to a psychologist at the hospital who was known to approve virtually everyone seeking transition. Then our doctor recommended feminizing hormones. At the time, I wondered if this was being done as a form of chemical castration.
She has seen over a thousand patients and is pointing to a single extreme shock story anecdote of someone who has experienced mental illness who came from an inpatient psychiatric unit. This person clearly has not “only seen one or two hours of therapy sessions” as some of the patients she alleges earlier. Instead, this trans youth has clearly gotten several evaluations from social workers, facility managers, and a psychologist. She did not assess this patient and was not involved in that, nor does she say how many assessments this patient received. She inserts her own opinion and her own interpretation of the situation here.
We also do not know what the result of this treatment was and if this person’s mental health saw improvements after treatment. Instead, we have her opinion that “this was done to chemically castrate this person.”
That same thought came up again with another case. This one was in spring of 2022 and concerned a young man who had intense obsessive-compulsive disorder that manifested as a desire to cut off his penis after he masturbated. This patient expressed no gender dysphoria, but he got hormones, too. I asked the doctor what protocol he was following, but I never got a straight answer.
As usual, she is misgendering this transgender patient. She claims that this patient expressed no gender dysphoria, but she does not claim to have personally assessed this patient. It is very possible that the patient was not forthcoming to her over the intake form, but was much more forthcoming to her doctors and therapists.
Another disturbing aspect of the center was its lack of regard for the rights of parents—and the extent to which doctors saw themselves as more informed decision-makers over the fate of these children.
In Missouri, only one parent’s consent is required for treatment of their child. But when there was a dispute between the parents, it seemed the center always took the side of the affirming parent.
She states that the center did not regard parents as having rights, and yet she points out that the clinic was directly following the law here. There is no allegation of wrongdoing here, only that she is upset that the center followed the law and allowed one parent to initiate medical care for their children based on best medical practices and guidelines. Missouri centers would likely not turn away a parent who was seeking care for their kid because they had experienced depression and needed an antidepressant either. If you follow the direction of all medical organizations and established research, the treatment of gender dysphoria does (and should) operate like other care in Missouri.
My concerns about this approach to dissenting parents grew in 2019 when one of our doctors actually testified in a custody hearing against a father who opposed a mother’s wish to start their 11-year-old daughter on puberty blockers.
I had done the original intake call, and I found the mother quite disturbing. She and the father were getting divorced, and the mother described the daughter as “kind of a tomboy.” So now the mother was convinced her child was trans. But when I asked if her daughter had adopted a boy’s name, if she was distressed about her body, if she was saying she felt like a boy, the mother said no. I explained the girl just didn’t meet the criteria for an evaluation.
Then a month later, the mother called back and said her daughter now used a boy’s name, was in distress over her body, and wanted to transition. This time the mom and daughter were given an appointment. Our providers decided the girl was trans and prescribed a puberty blocker to prevent her normal development.
This portion is extremely frustrating, because it seems that Jamie is upset that the doctors testified on a patient’s behalf that the best medical practices were followed. An entire court case happened around this proceeding where a judge weighed all of the evidence and statements and came to a verdict. We are supposed to put all of that aside because of a vendetta that Jamie has with her own place of employment.
I will highlight that in this case, she did not do the direct psychological assessment of the child. There are very simple reasons why she may have interpreted these events differently than how they actually occurred. For instance, on the initial intake, the parent may have not been given all of the information from the trans boy (again, she misgenders the patient). On the second visit, the parent may have provided more information that came as a result of the psychological assessment the boy gave.
This was likely explored in the court case, but Jamie wishes for you to take her interpretation of these events as true and wants to end care for an entire branch of patients because of that interpretation.
Because I was the main intake person, I had the broadest perspective on our existing and prospective patients. In 2019, a new group of people appeared on my radar: desisters and detransitioners. Desisters choose not to go through with a transition. Detransitioners are transgender people who decide to return to their birth gender.
The one colleague with whom I was able to share my concerns agreed with me that we should be tracking desistance and detransition. We thought the doctors would want to collect and understand this data in order to figure out what they had missed.
We were wrong. One doctor wondered aloud why he would spend time on someone who was no longer his patient.
Detransition is rare among trans youth – as mentioned before, it is only 2.5%. Interestingly, Jamie’s statements here do not allege any differently. Nowhere in her entire article does she state that there was an “explosion of detransitioners” or allege high numbers. This in a way confirms what we already know about the rarity of youth detransition.
One of the saddest cases of detransition I witnessed was a teenage girl, who, like so many of our patients, came from an unstable family, was in an uncertain living situation, and had a history of drug use. The overwhelming majority of our patients are white, but this girl was black. She was put on hormones at the center when she was around 16. When she was 18, she went in for a double mastectomy, what’s known as “top surgery.”
Three months later she called the surgeon’s office to say she was going back to her birth name and that her pronouns were “she” and “her.” Heartbreakingly, she told the nurse, “I want my breasts back.” The surgeon’s office contacted our office because they didn’t know what to say to this girl.
My colleague and I said that we would reach out. It took a while to track her down, and when we did we made sure that she was in decent mental health, that she was not actively suicidal, that she was not using substances. The last I heard, she was pregnant. Of course, she’ll never be able to breastfeed her child.
So instead of talking about high numbers of detransitioners or an “explosion” of them, like we often see alleged in anti-trans hearings, she instead focuses on single cases of detransitioners. This particular story is the only story of a detransitioner she can point to. I am sure she may have saw a handful of others, but given the dearth of detransitioners in her allegations, it would seem that her clinic was actually better at identifying youth who would be stable in their transition – otherwise she would be talking about how her clinic saw hundreds of detransitioners. Remember that anti-trans advocates claim that detransition rate is 85%, an easily disproven lie. See this tweet thread for my writing on this topic(click in and read the whole thread):
Erin Reed @ErinInTheMorn
Ever hear “80-90% of trans kids desist”? This is misleading and a lie. This comes from the DSM-4 criteria where any gender nonconforming kid was considered trans and counted under desistance. Likewise, trans kids COULD NOT transition and of course they “desisted.”
Here’s just one example: On January 6, 2022, I received an email from a staff therapist asking me for help with a case of a 16-year-old transgender male living in another state. “Parents are open to having patient see a therapist but are not supportive of gender and patient does not want parents to be aware of gender identity. I am having a challenging time finding a gender affirming therapist.”
I replied:
“I do not ethically agree with linking a minor patient to a therapist who would be gender affirming with gender as a focus of their work without that being discussed with the parents and the parent agreeing to that kind of care.”
All therapists who follow guidelines are “gender affirming.” This case manager, who is not a therapist herself, is advocating for trans youth to be sent to unaffirming therapists. In this particular case, the trans youth is concerned about not ending up in a conversion therapy situation – a very reasonable concern, especially with the advent of conversion therapy movements within the United Statestrying to target transgender people.
In all my years at the Washington University School of Medicine, I had received solidly positive performance reviews. But in 2021, that changed. I got a below-average mark for my “Judgment” and “Working Relationships/Cooperative Spirit.” Although I was described as “responsible, conscientious, hard-working and productive” the evaluation also noted: “At times Jamie responds poorly to direction from management with defensiveness and hostility.”
It sounds like she started getting negative reviews around the same time she started misgendering her patients and placing herself above the medical training of the doctors who work at the clinic as well as above the psychological training of their care teams.
Things came to a head at a half-day retreat in summer of 2022. In front of the team, the doctors said that my colleague and I had to stop questioning the “medicine and the science” as well as their authority. Then an administrator told us we had to “Get on board, or get out.” It became clear that the purpose of the retreat was to deliver these messages to us.
This is a good confrontation. As mentioned before, she is not a medical expert and does not do the in depth evaluation that the medical experts and psychological care teams do. Clearly she has a history of misgendering her trans patients. She saw herself as above best practices and medical guidelines. She elevates within her own mind the experience of edge case detransitioners and has given those with good results no credit and no voice.
The Washington University system provides a generous college tuition payment program for long-standing employees. I live by my paycheck and have no money to put aside for five college tuitions for my kids. I had to keep my job. I also feel a lot of loyalty to Washington University.
But I decided then and there that I had to get out of the Transgender Center, and to do so, I had to keep my head down and improve my next performance review.
I managed to get a decent evaluation, and I landed a job conducting research in another part of The Washington University School of Medicine. I gave my notice and left the Transgender Center in November of 2022.
Thank god she no longer cares for these patients.
For a couple of weeks, I tried to put everything behind me and settled into my new job as a clinical research coordinator, managing studies regarding children undergoing bone marrow transplants.
Then I came across comments from Dr. Rachel Levine, a transgender woman who is a high official at the federal Department of Health and Human Services. The article read: “Levine, the U.S. assistant secretary for health, said that clinics are proceeding carefully and that no American children are receiving drugs or hormones for gender dysphoria who shouldn’t.”
From her own letters, she shows that they were proceeding carefully and methodically. They identified cases of concern and the negative outcomes appear fairly rare given the over 1,000 patients she saw and the dearth of negative events. Furthermore, negative long term outcomes do not appear to be alleged in all but a couple patients out of the thousand patients she saw. Her own anecdotes do nothing to disprove this.
I felt stunned and sickened. It wasn’t true. And I know that from deep first-hand experience.
So I started writing down everything I could about my experience at the Transgender Center. Two weeks ago, I brought my concerns and documents to the attention of Missouri’s attorney general. He is a Republican. I am a progressive. But the safety of children should not be a matter for our culture wars.
Trans-exclusionary radical feminists often call themselves “liberal” or “progressive” but are anything but.
Given the secrecy and lack of rigorous standards that characterize youth gender transition across the country, I believe that to ensure the safety of American children, we need a moratorium on the hormonal and surgical treatment of young people with gender dysphoria.
I have already presented studies that show how many trans youth would take their lives if this happened. If she is truly concerned about her patient population, she would not advocate for this and against the medical science of dozens of the leading medical organizations.
In the past 15 years, according to Reuters, the U.S. has gone from having no pediatric gender clinics to more than 100. A thorough analysis should be undertaken to find out what has been done to their patients and why—and what the long-term consequences are.
Left handedness also exploded when left handed people were accommodated:
There is a clear path for us to follow. Just last year England announced that it would close the Tavistock’s youth gender clinic, then the NHS’s only such clinic in the country, after an investigation revealed shoddy practices and poor patient treatment. Sweden and Finland, too, have investigated pediatric transition and greatly curbed the practice, finding there is insufficient evidence of help, and danger of great harm.
It is so clear that she is working with the major anti-trans organizations in developing these calls to action. We have heard this in every Republican testimony for anti-trans bills this year. None of these countries have categorically banned gender affirming care for trans youth like she wants.
It is clear that anti-trans sources are using her testimony to attack gender affirming care nationwide for trans youth. I have no doubt that her story will be used to enact such bans in places like Tennessee, Texas, South Dakota, and Mississippi. Some of these bans will define gender affirming care as child abuse and take the kids of trans parents away. Let’s not gaslight ourselves into thinking that any of this is being done “for the good of children.” These policies have and will kill trans youth. Already, I have received four phone calls from the parents or friends of trans youth that have tried or completed attempts to take their own lives. That is the end goal of documents like this and anti-trans policies they add fuel to.
Please support my independent reporting and activism on transgender legislation by subscribing. You help me keep this going and keep people informed.
HERE IS ME, NOAHFINNCE, ANSWERING ALL THOSE UNCOMFORTABLE TRANS QUESTIONS THAT NOBODY WANTS TO ASK!! INVASIVE QUESTIONS! UNCOMFORTABLE QUESTIONS! TRANSGENDEREDLY ANSWERED!
I love this 23 / 24 year person. He is so open and honest. His personality is so energetic and engaging. There are days I can hardly focus yet his videos entertain me while educating me.
One of the reasons I am posting this video is when he talks about his body and sex along with how the person imagines themself or realizes them self during sex. Cis people don’t have to face this. People of any orientation who have not been abused or raped don’t have to deal with this. I do.
I am a gay man. I was abused during my childhood sexually and physically. How to reconcile my desire for being loved by men while fighting the horror of my abuse is something I dealt with not just most of my life but still today. How to take and enjoy the feelings of an act I want and agree with without triggering the memories of fear and horrible pain that it seems I can never forget. How to do the act that was used to hurt me in a loving way with a consenting partner is a mental struggle even now. Ron tells me I don’t have to keep asking if he is OK but in my head I am struggling with what is good or what is bad. AM I ABUSING THE ONE I LOVE LIKE I WAS ABUSED! Now Ron can touch me in bed when I am asleep without me reacting violently, but we are on our 33rd year as a couple. It is strange our cats could get all over me and I wouldn’t react but let Ron walk into the room or even while we are sleeping touch me and I reacted violently. I will soon be 60 and that past is a long time ago in history / terms of years but present far too often in my dreams even today. Last night I dreamed of my abusers and them hurting my cat to force me to agree to their demands. That was over kill on their part as they could have forced me anyway, they simply wanted to show they could take away anything I valued or loved.
Sorry this went far beyond where I wanted it to go. I enjoy this young man and his energy. I hope you will also. Plus he explains a lot of things that some cis people need to understand. Hugs
I would love to leave comments open on this post as I think many people will enjoy what Noah is presenting. Sadly, I don’t have the energy right now to monitor them and I know haters will want to argue debunked fringe shit. There was a time I loved that argument but right now my health won’t let me engage. I am getting better right now my heart rate is down from the high 140s to running in the 100s to 120s. I still am having a struggle with breathing but it maybe asthma or allergies, I still need a doctor to help me out with it. Right now the heart doctors have not responded, and the allergist appointment is late May. So much for health care in the wealthiest nation that just proposed another huge boost in military spending. I am like a wounded warrior going out to battle already deadly wounded. So I am going to again shut comments off. Trust me, I don’t like it. But I have had this video in the cue to post for a while. Notice the date of posting. I am really trying to bring as much information as I can, but I admit I am failing. Thank you. Hugs
I read the linked article and I suggest you do also. What this makes clear is that DeSantis wants is his own storm troopers, his own terror troops answerable only to him. The national guard is under the auspices of the US government and follows the polices of the Department of defense. The National Guard is part of the U.S. military but is unusual because it is controlled by both state and federal leaders. Most of the time, state National Guards are commanded by governors. However, presidents have the authority to call them into service to respond to hurricanes, bolster border security, and assist in overseas military operations.
Who will be the Commander in Chief of the Florida State Guard? Yes the ruler DerSantis himself. Total control total power. The white supremacist gang thugs Proud Boys, Oath Keepers, and the other far right gangs were the unofficial enforcement arm of the republican party. Now they will be wearing uniforms. Think of it!
The scary part is what DerSantis claimed about his new personal army. “The Florida State Guard will be comprised of Floridians, and it will be assigned to assist and help only Floridians,” DeSantis said in a news conference last June. “It will not be subject to be mobilized by the federal government, and the federal government cannot impose policies or penalties on the Florida State Guard.”
In other words, just the right kind of people will be allowed to join. Will that mean just white people? Will it mean only Christians? Clearly no gays, lesbians, or trans people will be allowed. Also you know those annoying rules that the Federal government has for fairness, use of force, medical readiness, and the things the force can be used for all are gone, now ruled by people who claim vaccines are more dangerous than the diseases they help prevent, that claims adamantly that the 2020 election was rigged and stolen somehow but have no evidence of it, that claim that drag queens readding to kids is sexual abuse, that not enforcing stereotypical gender roles from the 1950s is sexualizing kids, and that teachers are groomers while ignoring the many religious leaders charged with sexual crimes against kids. And so much more.
The ruler of Florida will now have his own goon squad fake white supremacists Christian nationalist to intimidate the governors enemies and it enforce his decrees in the state. And he wants to be kind of the entire country not just Florida. Will these troops be assigned to minority area voter places under some fake guise of “keeping the peace”? Will they show up at school board meetings in progressive areas to express the displeasure of the governor? Will they have the authority to make the arrests demanded by the king of Florida that is not quite legal for the police to do? Just how far into fascism do we have to before people see the danger. trump just started the ball rolling in to the 1930s Germany, DerSantis wants to finish recreating that time here. Seriously this needs to be fought with all we have. Hugs
As lawmakers in Tallahassee consider Gov. Ron DeSantis’ budget proposal this session, they will be also be deciding whether to approve a steep funding increase establishing Florida’s own branch of the military. The state guard was dismantled at the end of World War II.
“The Florida State Guard will be comprised of Floridians, and it will be assigned to assist and help only Floridians,” DeSantis said in a news conference last June. “It will not be subject to be mobilized by the federal government, and the federal government cannot impose policies or penalties on the Florida State Guard.”
In its first year, the legislature approved $10 million to restart the Florida State Guard. DeSantis now wants to increase that to $98 million this year.
“The Florida State Guard will be comprised of Floridians, and it will be assigned to assist and help only Floridians,”***
***Unless those Floridians are gay, trans, in a same-sex marriage, vote Democratic, are Black, ex-convicts, undocumented, straight, but want their kids taught accurate history or enjoy drag shows.
Well, first of all there’s us. First the drag queens, then the rest of the gays, then anyone Republicans don’t like…except for the Jews. They still need them to bring on the rapture.
So if he gets his own army, that helps only Florida, then there will be no need for any assistance from the National Guard in case of a hurricane or any other emergency. He’ll spend all his money on his hate, but he’ll have his hand out in an instant if anything goes wrong.
The building of his own SS troops before the Fascism take over the country. Who needs to go to Argentina to hunt for the good old Nazis when Florida is just right there.
At this point, we need Governor Newsom, Governor Hochul, and Governor Pritzker to form a pact to each do everything Florida does. DeSantis targets Disney? Newsom, Hochul, and Pritzker go after Hobby Lobby and Chick-fil-A. DeSantis tells the College Board they have to bow to his “anti-woke” bullshit or be kicked out of Florida? Newsom and Hochul tell the College Board that if they do, they’re banned from California, New York, and Illinois. DeSantis wants a private army in Florida? Looks like California, New York, and Illinois need private armies, too. Make sure the Republicans in the federal government know that if they allow this shit, they’re signing off on blue states doing it too. DeSantis is engaging in the social equivalent of unilateral nuclear proliferation. It’s time for Democratic elected officials to get M.A.D.
the federal government cannot impose policies or penalties on the Florida State Guard
What BS, there will be all kinds of employment regs you have to follow. And it is just another state police force (militia) that has to follow the Constitution.
This is the first concrete step to his ultimate plan for Florida to secede. His plan goes far beyond running for president. 162 years ago — “On January 10, 1861, Florida delegates who were meeting in the state capital, Tallahassee, voted to secede from the U.S. Florida became one of the six original Southern states to form the Confederate States of America.”
As the complete Article states, the Florida National Guard is “insufficient”, because it’s under Federal control. This is once again posturing by a short heavy wannabe Presidential hopeful. Who thank dog is term limited as Governor , after we send him packing should he gain the nomination for President
And now he’s forming his own army, probably to fend off the next war of northern aggression. I’m reminded of this scene in The Great Dictator: https://www.google.com/sear…
Tut, tut. Those are subject to mobilisation from the Federal Government, and can be sent to other states by the Feds. This would be Sandtits’ personal army.
Aron Ra was answering questions from a right wing troll who demanded he answer a question of gender and biological / assigned at birth sex. Ra brings in an expert that points out the medical science as we know it now. The part runs until about 22:15 at which point the guy asks questions about morals I also found interesting. But the main part I wanted everyone to see is the debunking of the idea that biological sex can be determined by looking and is strictly binary, because both of those ideas are just wrong medically. Biologists and medical science clearly show that sex is a spectrum and that gender is not tied to if it dangles or not. Also I have decided to shut off comments as I cannot moderate the misinformation at this time.
If you want to talk about the post and your feelings while admitting the science the majority of medical organizations agree with, just email me. I will read it even if you don’t get a reply. If you want to argue conspiracies or weird claims based on faulty studies or fringe doctors / Florida Health Department crazies, then don’t bother emailing me. I won’t read it, won’t bother responding. Right now I am done trying to show the anti-trans anti-progressive social policies how they are wrong. They cannot deal with reality and I cannot help them at this point. Time has moved forward; social progress has been made and they cannot deal with it for whatever reason. So they want everyone to go back to the time they were comfortable with the way things were. Traditionalist. It was good enough in the old times, why not good enough now? The simple answer is we know more now than we did then. Hugs Email is Scottiestoybox@gmail.com
I tried to group these articles in some sort of order. But you can see the goals of the right just from the titles. The eradication of transpeople at any age from society. The removal of any gay rights with the goal of eradicating gay people from society. The enforcement of stereotypical gender roles and the returning to the days when women were dependent on men, and few had authority or independence on their own. They want tyranny and dictatorship of one party rule with no restraint on their activities even to the point of attempting the overthrow of the US constitution / government and the celebration of those that committed the illegal acts in the coup attempt. Republicans want to rule not govern, they want to have the people afraid to disagree with them or dare to speak against their rule. Just like the countries of China, North Korea, and their beloved Russia. Please notice the attempt is to return the US to the regressive oppressive times before the New Deal that empowered the public. They want 1910 to 1920. We had better join together to stop them or we won’t be able to. DerSantis is shopping the campaign slogan “Make America Florida”. Is that not enough of a threat to the country? Has the trump years not shown how quickly the right can move if given power to destroy all norms and rights to enforce their minority rule. McConnell even said that while republicans will lose elections the democrats couldn’t stop a republican stacked court system from enforcing republican goals for decades. He was correct. Mitch McConnell said, “My goal is to do everything we can for as long as we can to transform the federal judiciary, because everything else we do is transitory.” Hugs
Read the comments on this to see how things used to be for families and kids before labor laws and government assistance were created.Kids younger than five working a full day in the farm fields. Is this the grand vision of the future the country needs or wants? Think of every movie of the future that has a great working society and they are progressive but the ones with dystopian unfair or dangerous future and it is regressive oppressive hellish places were greed is king with businesses in charge killing any regulation that prevents profit. Hugs
Again these bills are a way Christians can force their moral views on everyone, a way they get to rule on how every person gets to live their lives. It gives these rabid fundamentalists Christian republican groups the right to tell everyone else what they can do, regulating what everyone can watch / read in order to conform to a strict religious view of morality written 2,500 years ago. It ignores all medical, scientific, and social advances done in the years since their holy books were written and mistranslated. Society has advanced as human understandings have, yet these oppressive regressive people want to ignore all that. Would they also like to go back to the medical understandings in the 1600s, 1700s, or even what was known medically in 1900. That was 28 years before penicillin was discovered. 21 years before insulin was discovered. Tell me if their holy book written knew everything about morals why did it support slavery? Do we return to that also to please Christian fascists? This is an attempt to enshrine a religious morality over everyone regardless of if you belong to that or any religion. Again it is not about these people being able to live and act as they wish, it is about forcing everyone else to live by their church rules / doctrines. Hugs
Bills are part of religious right’s post-Roe strategy, with most prevalent ones relating to age verification of sex-related websites
A wave of proposed legislation pushed by Republicans across the US at the state level is aimed at outlawing aspects of sexuality that could have a huge impact on Americans’ private lives and businesses.
Opponents to the laws before legislatures in various states say the planned new legislation could spawn prosecution of breast-pump companies in Texas for nipples on advertising, or a bookstore might be banned from selling romance novels in West Virginia, or South Carolina could imprison standup comics if a risqué joke is heard by a young person.
The bills are part of a post-Roe nationwide strategy by the religious wing of the Republican party, now that federal abortion rights have fallen. They range from banning all businesses that sell sex-related goods to anti-drag queen bills. Tyler Dees, an Arkansas state senator who wrote an anti-porn bill said: “I would love to outlaw it all,” referring to porn.
The most prevalent bills relate to age verification of sex-related websites. Seventeen states drafted porn age-verification bills, many inspired by Louisiana’s law that went into effect in January. Louisiana’s law requires websites featuring 33.33% or more pornographic content to check government-issued ID to verify users are 18 and older. Websites that don’t comply face civil penalties. Parents can sue the site if kids access it.
In Texas, a new bill requiring age verification on websites with pornographic content defines images of the female breast “below the top of the areola” as porn, potentially hitting at business advertisements. In West Virginia, a bill outlawing all sexually oriented businesses is on the docket, with a definition that includes art studios with nude models and wrestling arenas. In South Carolina a bill would criminalize using “profane language” related to “sexual or excretory organs or activities” in front of minors during performances. The punishment? Up to a decade in prison.
Some bills define porn so broadly that anatomy textbooks or sex education websites would meet them.
“I don’t think such laws for the internet are constitutional,” said Eugene Volokh, a professor of Law at UCLA.
Laurie Schlegel, a Republican state senator who drafted the Louisiana law, is a sex-addiction therapist educated at Baptist seminary, who opposed transgender students from being on sports teams that align with their gender. Schlegel’s anti-LGBTQ+ views fit with the broader goal of the laws, according to Carolyn Bronstein, a professor of media studies at DePaul University.
“These laws are really not about controlling minors’ access to violent pornography … In the conservative world view, pornography is information about LGBTQ identity, abortion, gay marriage,” said Bronstein.
Eight states have justified their actions by saying that porn is “creating a public health crisis”. Louisiana’s bill claims that pornography “may lead to low self-esteem, body image disorders, an increase in problematic sexual activity at younger ages … impact brain development … shape deviant sexual arousal, and lead to difficulty in forming or maintaining positive, intimate relationships, as well as promoting problematic or harmful sexual behaviors and addiction.”
Historian Whitney Strub, an associate professor of history at Rutgers University, doesn’t think these ideas are well-founded. “Framing pornography as a public health crisis is not driven by serious engagement with the social scientific literature,” he said. “They’ve even got fake peer-reviewed journals that give the imprimatur of scholarship … It’s been a very smart rebranding of evangelical Christian conservatism.”
Why are all these bills being proposed now? Strub thinks it’s partly because of the overturning of Roe v Wade. “Abortion gave a certain coherence to conservative politics in the United States. And it certainly still does … but they’re in the position of Ahab if he slayed the white whale … I mean, there’s no more Moby-Dick.”
There is hypocrisy on display also.
In many of the states where the anti-porn bills are being put forth, minors can legally have sex and get married. “In Louisiana, you can have sex when you’re 17 with a person in their 30s, but you can’t watch porn,” said Jason Kelley, associate director of digital strategy for the Electronic Frontier Foundation.
In Mississippi, Arkansas and Louisiana, the age of consent is 16. With parental permission, Mississippi allows 15-year-olds to marry, Louisiana 16-year-olds, Arkansas 17-year-olds, and West Virginia kids of any age.
Dees, who wrote Arkansas’s age verification bill, a copycat of Louisiana’s, said porn causes depression and anxiety, divorce and “permissive sexual attitudes” and infidelity. “When I think about the children … I want to protect their innocence,” Dees said.
Strub said this is an old trope: “The political figure of the innocent and imperiled child just has a never-ending purchase on American politics … [it] essentially shuts down debate because it immediately creates a binary in which anybody who disagrees with you is [a] perverted groomer.”
Dees is also the co-author of anti-drag queen legislation in Arkansas, that classifies drag performances as the same category as pornography. “It’s not really a meaningful distinction to [conservatives]. They’re both sexual degeneracy in its different guises,” Strub said.
Dees claimed that his porn verification law “doesn’t have anything to do with any political messaging. It has to do with exposure to material that is harmful, period … There’s a clear enemy in the smut-peddling garbage that’s online.”
But measures already exist to prevent children accessing porn. “There’s a really easy way to keep kids from accessing adult content. And that’s a device-level filter” on mobile phones that block adult websites that are registered as Restricted to Adults, said Mike Stabile of the Free Speech Coalition, which advocates for the rights of sex workers.
These laws, according to Stabile, aren’t going to stop kids from looking at porn. “Even if they were to block all sites, you’re still going to have adult content on Twitter and Reddit … kids will get VPNs,” he said.
Stabile thinks we’ll see up to two dozen age-verification bills introduced by the end of the year.
Dees hopes he is right and has eyes beyond the state level eventually. “My prayer is that enough states continue to push for this measure, and that we send a loud enough message where federal law can be put into place,” he said.
Enlarge/ A woman watches white flags on the National Mall on September 18, 2021, in Washington, DC. Over 660,000 white flags were installed here to honor Americans who have lost their lives to COVID-19.
Americans spend an exorbitant amount of money on health care and have for years. As a country, the US spends more on health care than any other high-income country in the world—on the basis of both per-person costs and a share of gross domestic product. Yet, you wouldn’t know it from looking at major health metrics in years past; the US has relatively abysmal health. And, if anything, the COVID-19 pandemic only exacerbated the US health care system’s failures relative to its peers, according to a new analysis by the Commonwealth Fund.
Enlarge/ Health care spending of high income-countries by share of GDP.
Compared with other high-income peers, the US has the shortest life expectancy at birth, the highest rate of avoidable deaths, the highest rate of newborn deaths, the highest rate of maternal deaths, the highest rate of adults with multiple chronic conditions, and the highest rate of obesity, the new analysis found.
“Americans are living shorter, less healthy lives because our health system is not working as well as it could be,” Munira Gunja, lead author of the analysis and a senior researcher for The Commonwealth Fund’s International Program in Health Policy and Practice Innovation, said in a press statement. “To catch up with other high-income countries, the administration and Congress would have to expand access to health care, act aggressively to control costs, and invest in health equity and social services we know can lead to a healthier population.”
Dying young
Overall, the analysis paints a grim picture of how much catching up the US has to do. In terms of life expectancy, the US has trailed its peers for years but took a nosedive during the pandemic, while other countries fared better. In 2020, the average life expectancy at birth in the US was 77 years, three years lower than the average for high-income countries. The next lowest life expectancy among high-income countries was from the UK, which had a 2020 life expectancy at birth of 80.4 years.
Provisional data for 2021 suggests US life expectancy fell nearly a full year further, from 77.0 years to 76.1 years. Relatedly, the US had the highest rate of deaths from COVID-19 in 2020 compared with its high-income peers and was among the lowest of its peers in rates of COVID-19 vaccination.
In a particularly shameful set of statistics, the US continues to have the highest infant and maternal mortality rates of any other high-income country. In 2020, there were 5.4 infant deaths per 1,000 live births in the US, while the average among high-income countries was 4.1 infant deaths. In Norway, there were 1.6 deaths per 1,000 live births. The health care system is also failing mothers. In 2020, there were 24 maternal deaths per 100,000 live births, about 2.5 times higher than the average for high-income countries. The country with the next highest maternal mortality rate was New Zealand with 13.6 per 100,000 live births.
Enlarge/ Rates of infant and maternal mortality among high-income countries.
With many US states now rapidly turning back the clock on reproductive rights and maternity care, the US’s appallingly high rates of infant and maternal deaths are expected to worsen.
Beyond pregnancy, Americans are dying from other conditions that are treatable or preventable at a rate far higher than those seen in all other high-income countries. In 2020, 336 US deaths per 100,000 people were avoidable, while the average among high-income countries was just 225 deaths per 100,000. The rate of avoidable deaths has been rising in the US since 2015, the analysis notes.
Sicker
That tracks with the finding that Americans are more likely than their high-income-country peers to have multiple chronic conditions. In 2020, 30.4 percent of US adults said that they had previously been diagnosed with two or more chronic conditions in their life. Among other high-income countries, no more than a quarter of adults reported having two or more chronic conditions. America’s high obesity rate may play into that discrepancy. The US has a higher obesity rate than any other high-income country. In fact, it’s nearly two times higher than the average of its peers.
While Americans are dying young from avoidable conditions, they’re also spending an exorbitant amount on health care. The US spent 17.8 percent of its GDP on health care in 2020, nearly twice as much as the average of 9.6 percent among high-income countries. On a per-person basis, it outspent its peers, paying nearly $12,000 per person via government insurance programs, private insurance coverage, and out-of-pocket costs. The country that came the closest to US spending was Germany, with a little over $7,000 per-person spending.
The data hints that these high prices are discouraging Americans from getting the care they need, potentially feeding into the country’s high rates of chronic conditions and avoidable deaths. In the analysis, the US had among the lowest rate of doctor visits, with just four per year. The average was 5.7. The US also has one of the lowest rates of practicing physicians per 1,000 people—2.6 per 1,000, while the average is 3.7.
The US was the only high-income country in the analysis that does not guarantee health coverage. People in most other high-income countries have guaranteed health coverage with the option of buying supplemental private coverage.
I have been reporting on this for years now as the article says “…describes the current political landscape as a “war against LGBTQ people in America and their very right and ability to openly exist.” These laws have nothing to do with protecting children as they claim but instead are attempts to force regressive religious morality on the entire country by a minority who don’t feel comfortable with “those people” and want them removed from public view / discussion. With every push to return the country to the society of 100 years ago which rolls back every advancement in civil rights that have been achieved, these people are emboldened to push harder to oppress more people into living the way that maga Christian minority insists they have a right to force everyone else to live as. It is not enough for them to live as they wish, they insist you live the way they do also, that you believe as they do, that you follow the moral dictates written 2,500 years ago for a culture long gone. But it is not enough for these people and never will be until they are in charge of and get to rule over every aspect of your life. Allies of the LGBTQ+ we need to you stand up and add your voice to protect the rights of minorities, women, and the LGBTQ+. Hugs
Today’s heart rate readings have seen an improvement. The lowest it has been is 95 the highest sustained was 136 with the average so far of 126 bpm. So I am getting better. Still no call from the heart doctor’s office so Monday I will call them. This has been going on for too long and too dangerous, not to mention causing me to struggle to function. Hugs
Trans-rights activists protest outside the House chamber at the Oklahoma State Capitol on Feb. 6, 2023. (SUE OGROCKI/AP)
From bills in legislatures to restrictions in schools and health care, growing rhetoric throughout the US is part of a “full-out attack” against LGBTQ+ people, advocates say.
The volume and speed of anti-LGBTQ+ bills advancing through state legislatures has already defined 2023 as a historically challenging and frightening year, advocates say.
In a new report, the Movement Advancement Project (MAP), which tracks LGBTQ+ policy, describes the current political landscape as a “war against LGBTQ people in America and their very right and ability to openly exist.” It is a culmination of efforts: gender-affirming care bans for trans youth becoming law in states where such bills were previously blocked, growing efforts to restrict how students learn about LGBTQ+ subjects in schools, an increase in dehumanizing rhetoric that could lead to harassment or violence.
“I’ve been working in the movement for 15 years,” said Naomi Goldberg, deputy director and LGBTQ program director at MAP. “To me, this is a different moment. … It is hard to see this as anything but a full-out attack and full-out war on LGBTQ+ people when you look at all of the areas of life, at all of the parts of our communities that are being attacked.”
The Human Rights Campaign (HRC), the country’s largest LGBTQ+ organization, sounded similar alarm bells earlier in the week. The organization has so far tracked 340 introduced anti-LGBTQ+ bills, including the most anti-transgender bills ever filed that the group has seen.
Those bills include ones that would prohibit students from playing school sports that match their gender identity and bills that would restrict gender-affirming medical care for minors. Over 90 bills targeting medical care for trans youth have been filed so far, according to the HRC’s count. South Dakota and Utah have already signed such bills into law, while states like Tennessee and Mississippi are quickly moving similar bans through their legislatures. Other proposed bills direct school employees to effectively misgender students, mandating that students are referred to with pronouns that match their sex assigned at birth unless a parent intervenes.
“This situation is terrifying. It’s scary and it’s harmful. We know last year was bad. … we anticipate this year being historically bad,” Kelley Robinson, the president of HRC, said on a Tuesday press call with reporters.
Within the past three years, “firsts” in anti-LGBTQ+ bills have piled up, MAP’s analysis finds: the first legislative ban on trans youth playing sports that match their gender identity in Idaho, the first legislative ban on gender-affirming medical care for trans youth in Arkansas, the first state ban on the use of X as a gender marker on identity documents in Oklahoma, and the first “Don’t Say Gay” law passed in 20 years in Florida.
Efforts outside statehouses are another part of what make the current moment unique, per the report — including child abuse investigations ordered by the state of Texas against families seeking gender-affirming care and Florida’s board of medicine moving to restrict such care for trans youth.
Some LGBTQ+ advocates are concerned about the potential for new anti-trans bills to restrict whether families can seek gender-affirming care in other states if their own state bans the care. In Oklahoma, one bill prohibits doctors from making a referral to “any physician or health care professional for gender transition procedures” for patients under 18. The consequences of such a referral would be meted out by the state, which would have jurisdiction over its own doctors. However, since any referrals would have to be for out-of-state care, it still has the potential to limit interstate travel for gender-affirming care, said Logan Casey, senior policy researcher and adviser for MAP, over email.
More bathroom bills, which aim to restrict how trans people are able to use the bathroom that matches their gender identity, are filed this year than in previous years, per the Human Rights Campaign’s count — and fewer bills targeting how trans students can participate in sports are being introduced.
Even when the legislation doesn’t become law, it still causes harm, Olivia Hunt, policy director at the National Center for Transgender Equality, stressed during the call. Hunt pointed to a recent poll that found 86 percent of surveyed trans and nonbinary youth said that debates around state laws restricting LGBTQ+ rights for young people negatively impacted their mental health.
“Trans youth are making their way through an already difficult world, where they’re trying to understand who they are … and on that journey, they’re vulnerable, and they deserve the love, respect and support of their communities. Instead, they’re portrayed as someone to be feared, controlled or erased,” Hunt said.
The Biden administration has vocally supported LGBTQ+ rights, directing federal agencies to roll back Trump-era policies that advocates denounced as discriminatory and prioritizing data collection on LGBTQ+ experiences. Goldberg said she wants to see enforcement of federal protections from the Biden administration. Those include the Department of Health and Human Services’ proposed rule to restore protections for gender identity and sexual orientation under the Affordable Care Act, and Title IX protections proposed by the administration that would apply to trans students. Following Biden’s State of the Union address, HRC called on the administration to finalize both of those rules.
“I think it would be great to have more leadership,” Goldberg said.





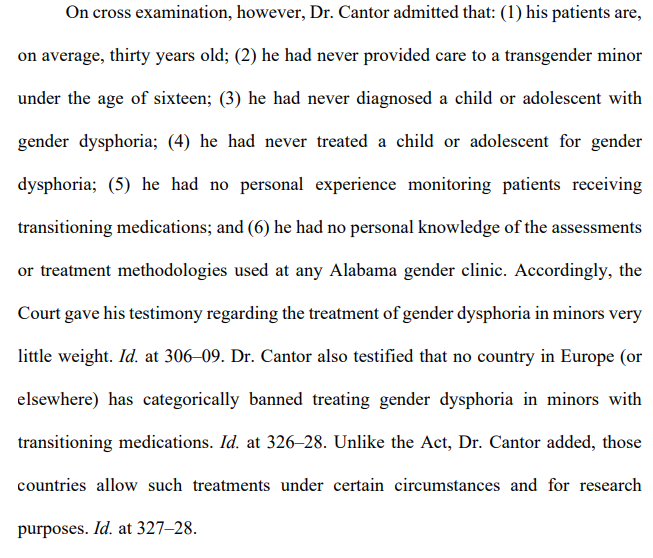


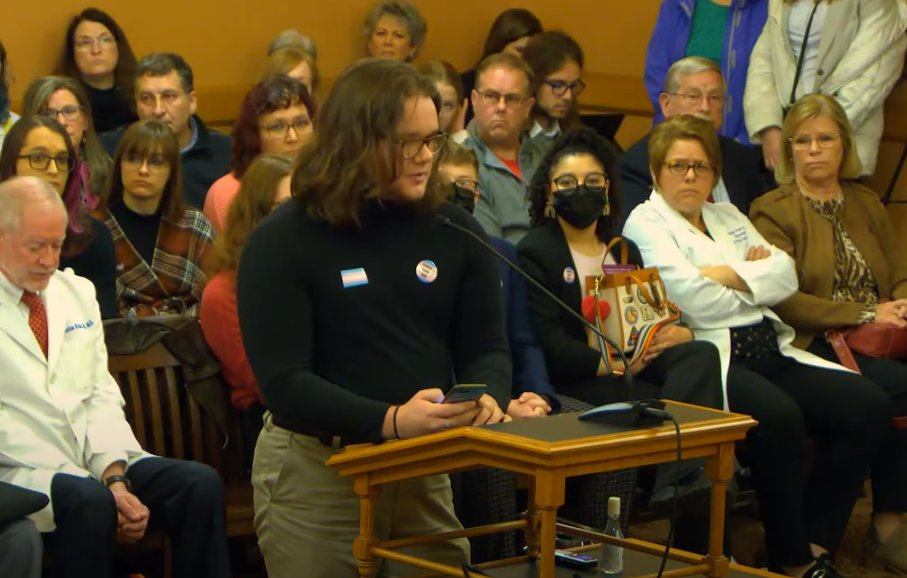
















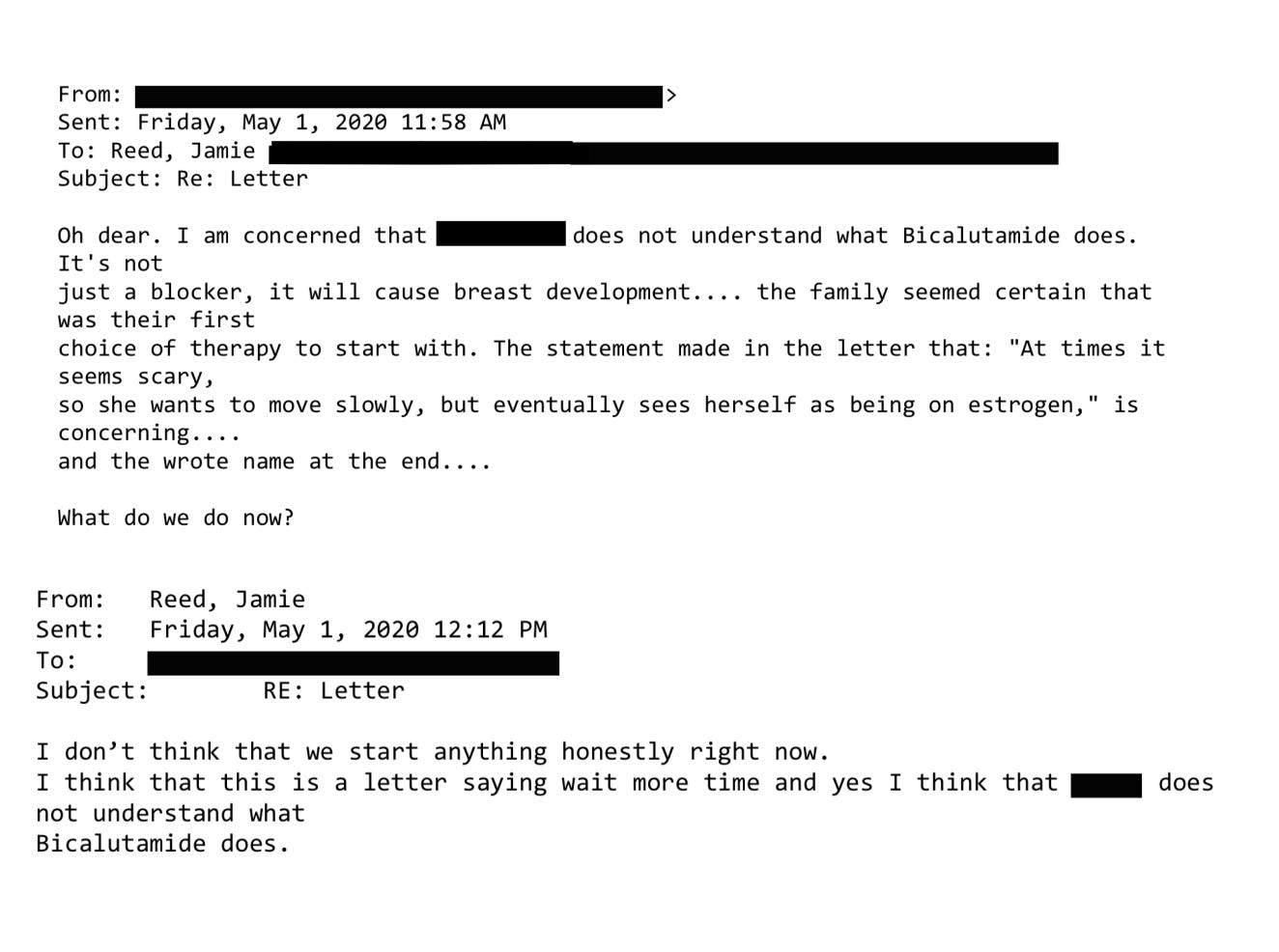
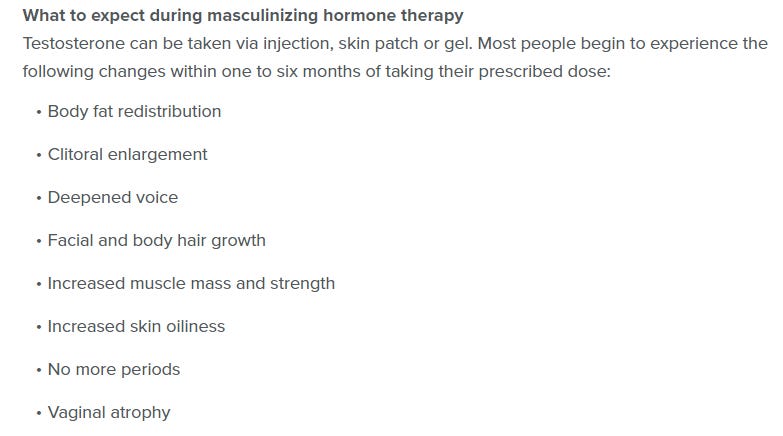
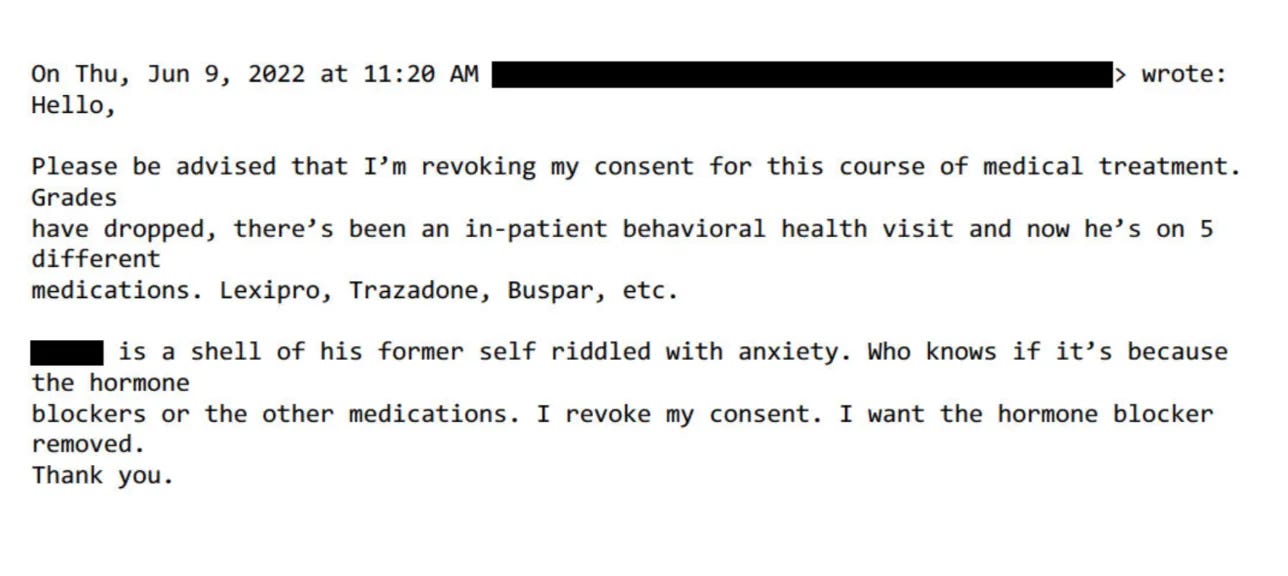
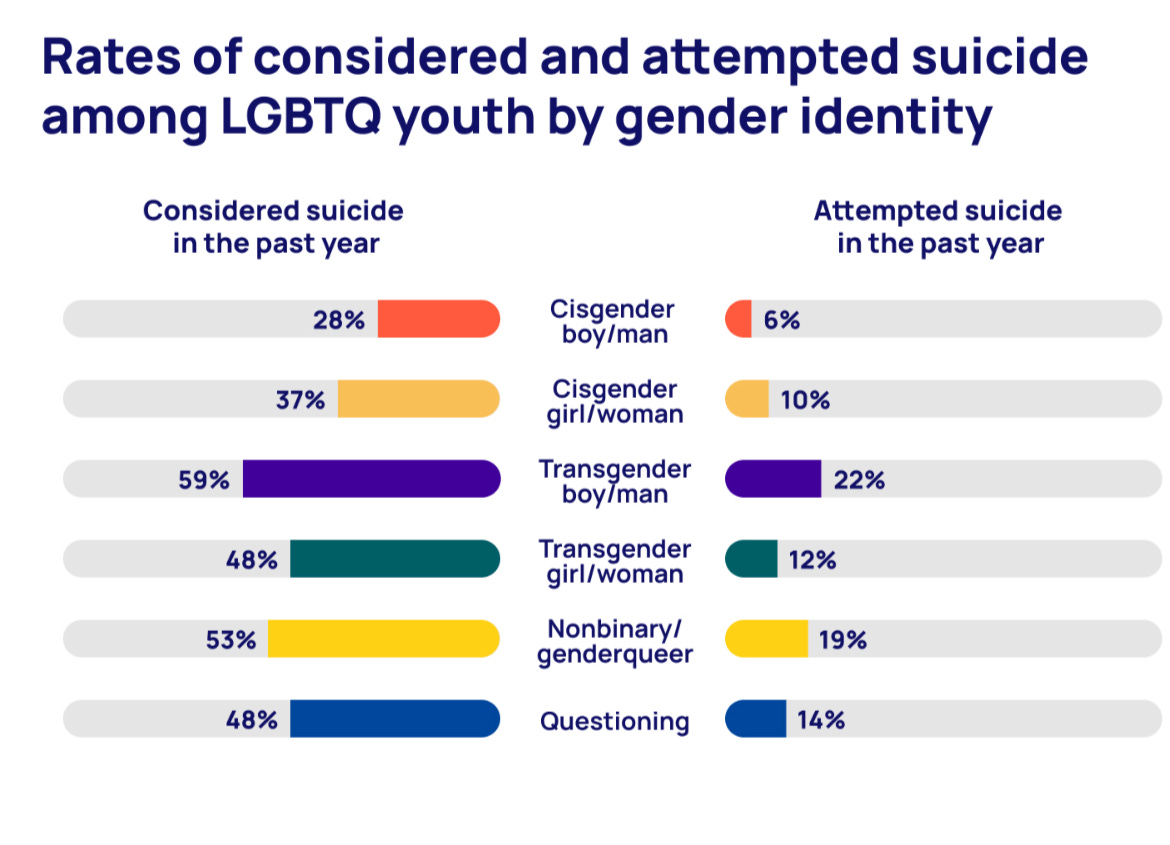








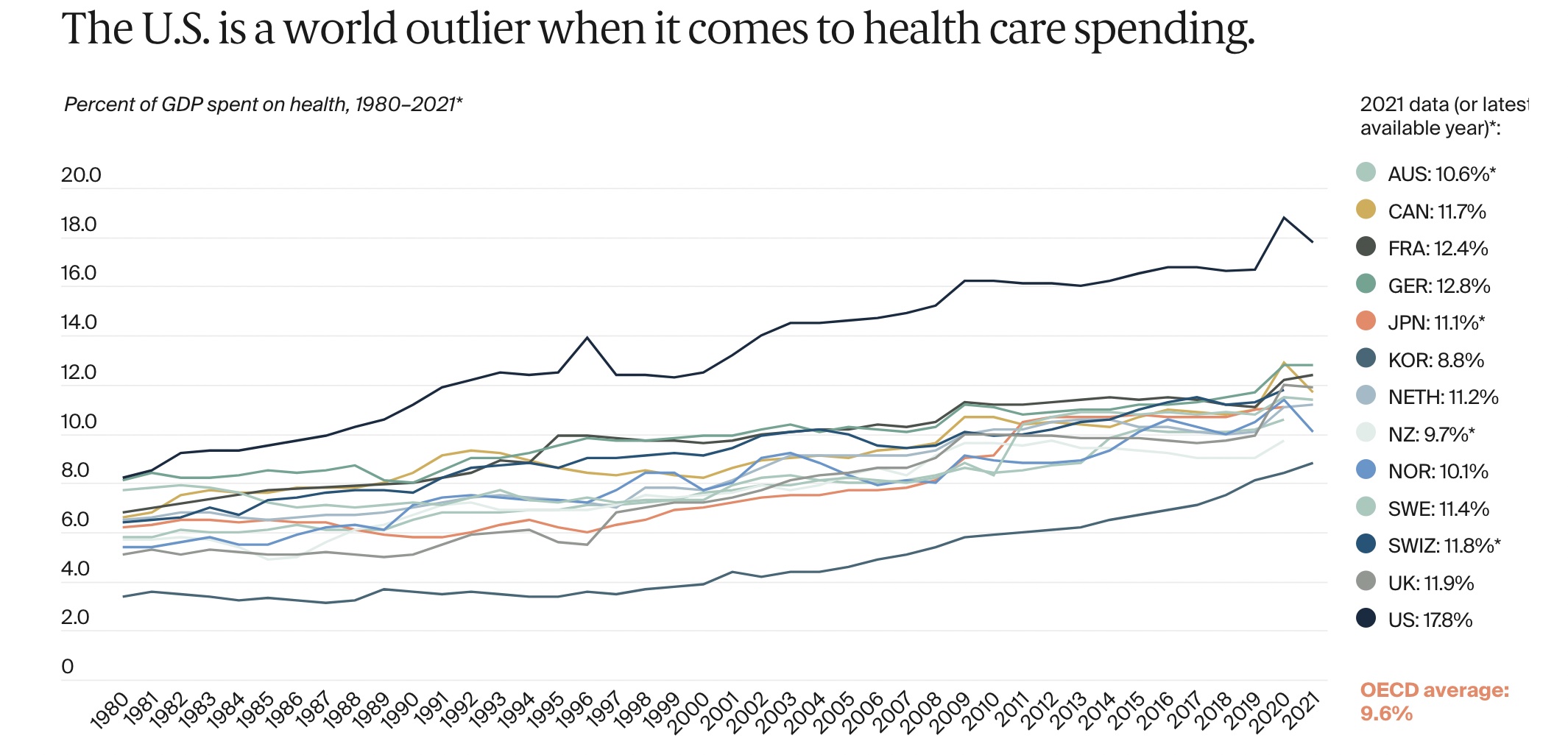
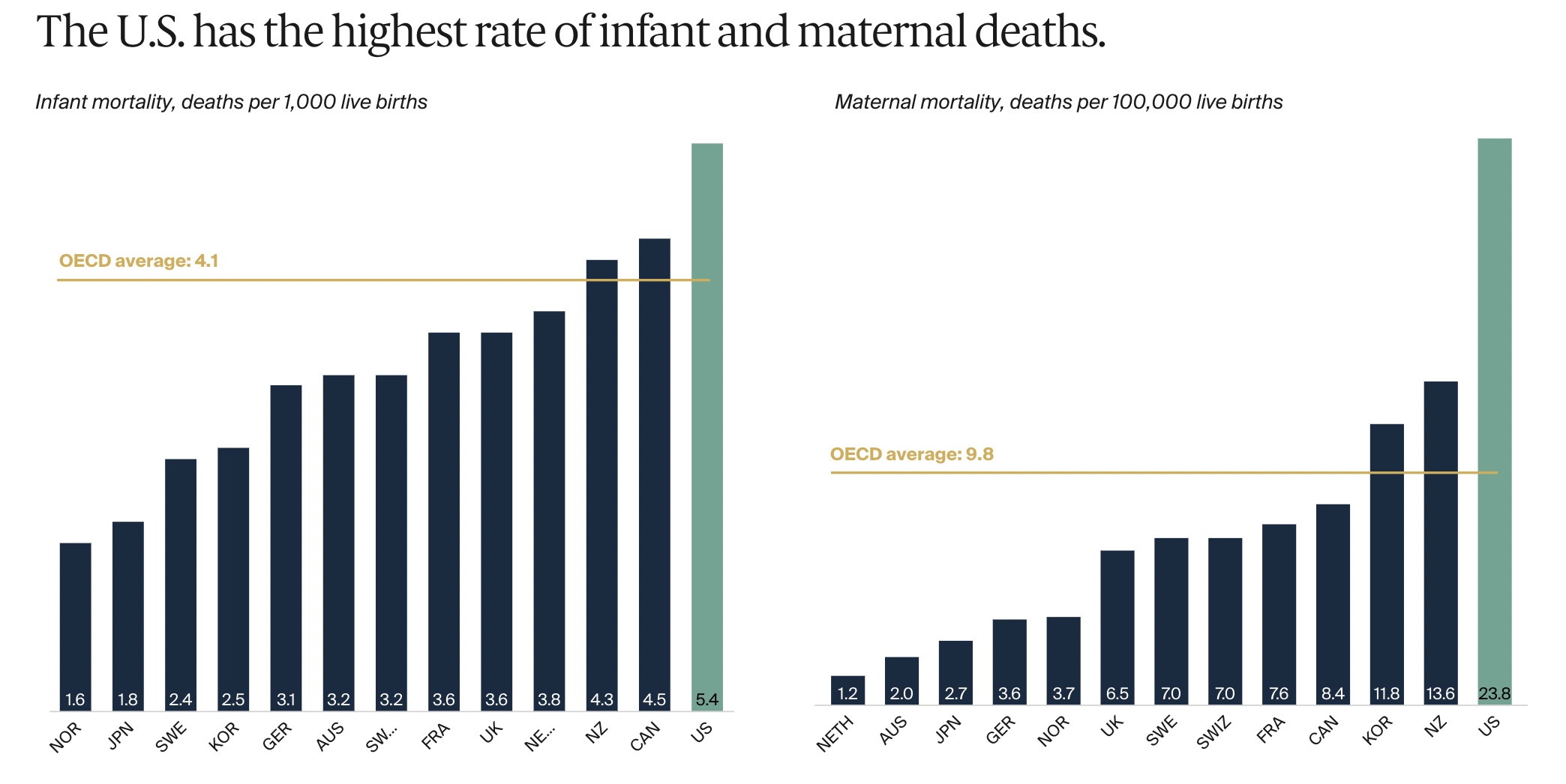











{kind=link}