I have been really struggling lately. I keep saving comments to answer later that days go by I don’t get to. I keep saving them so I can reply. I have not announced it here on the Play Time but I finally made an appointment with a therapist.
When I made the appointment they asked a few questions and then tried to get me to come in the next morning. I said no. I just couldn’t deal with it. On top of the car just needing a new engine for 4 grand due to a faulty temperature sensor we had the van checked. It is 17 years old. It has a lot of small stuff wrong but each fix adds up and the total was two grand.
I am hardly sleeping and during the day the intrusive thoughts can get me struggling and crying. So what should only take me a few hours ends up taking me 6 to 8 hours. It is even more frustrating because my attention deficit disorder has increased to the point I can lose track of what I am doing or get switched over to something else almost without noticing so that I get pulled down rabbit holes until I see it.
Also I find sitting at the computer gets painful so I get up and do things like the dishes. Sadly I drive myself to the point I can’t stand or are near collapse. That happened last night. Ron was doing other things so I had the night before promised to take a small amount of mashed potatoes left over and fry it along with making him scrambled eggs. Then I did dishes at noon and right after I made a red sauce. I was exhausted and not able to stand by the time I got it done. Ron put the red sauce aside and made us the planned supper of chicken, pork, and beef chopped up for fajitas. But I could hardly eat.
Then Ron found me falling asleep at my desk I was so tired. Ron asked me as he helped me to get my nighttime meds and go to bed, Ron asked me if I had managed to get to the comments I had told him I saved. I just sighed. I told him I still have them saved and will get up in the morning and reply to them. I did not do that. I used to jump out of bed fully energized which always amazed Ron. Now I struggle to get up, often laying there for several hours hoping to go back to sleep. In the past I would get up in the middle of the night if I couldn’t sleep, but now I just lay there desperately hoping to sleep without a nightmare.
But this is not what this post is about.
I use a name not used by my abusers. The name they used for me was a slave name. You can see it used for one of the prominent characters in Roots. It was used to make me an it. I was often told how I got my name at age three. My first real memories are a bus ride next to a woman I did not know. I am told when she introduced me to the “family” one of my hell spawn female siblings ask “What do you call IT“ My new adoptive mother gave me the name normally given to slaves in the south as I understand. I never used it personally and hated it all my life.
Ron never used it even though they tried to get him to do so. They would use it to him to refer to me and he would pretend to not know who they were talking about. I guess good for me the name was not the one used on my birth certificate so as I got to move beyond their influence I could use my birth name and then when I got away from all their ability to influence or threaten me I modified my birth name to what I felt most comfortable. See the only time they used the real name was to mock me and so when I got the chance to choose my name for myself I did.
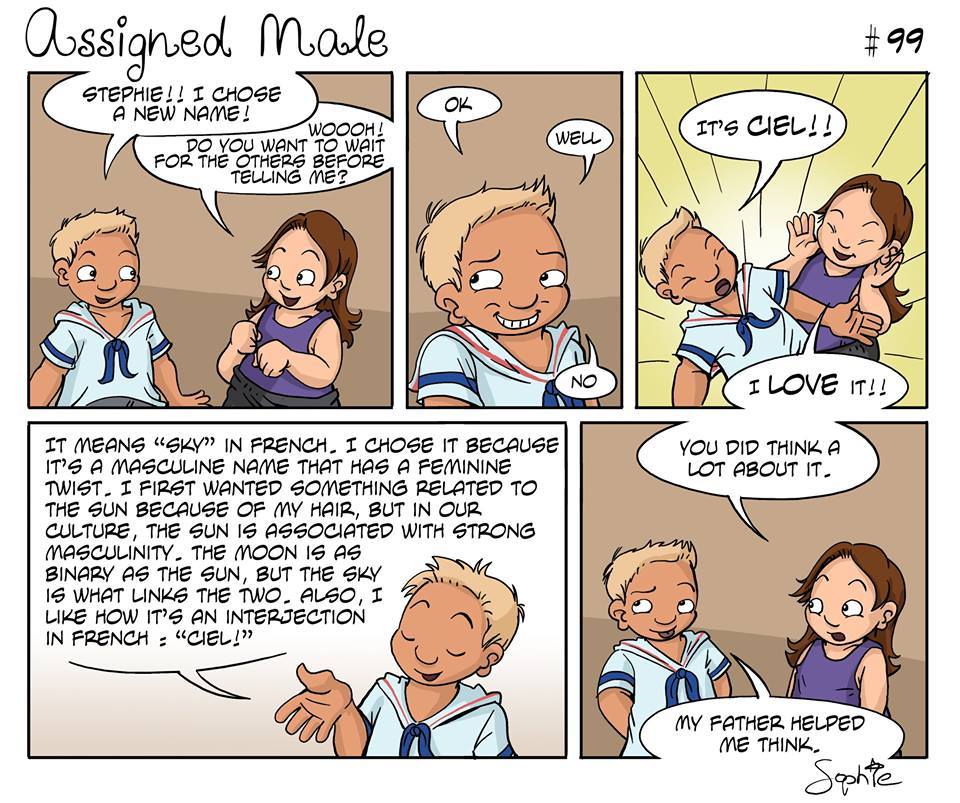
I am Scottie !!!
I love who Scottie is and think he is done very well with the life hand he was dealt. But all this is to explain why the series of cartoons by Sophie Labelle are so important to me. So here is the one by her that jogged me to make this post. I had tried to restrict posts about my abuse. But this was so on point I knew I had to do so. Sadly I had no father or other to help me find it, they hated that I demanded they call me by it. It caused me to hang up on them repeatedly when they would call me by my abused name. They finally did adjust when in their old age they needed me to help them. Hugs
At the South Louisiana Ice Processing Center in Basile, detainees say they were forced into hard labor – and sexually assaulted and stalked by an assistant warden
‘It is for my daughter and my family that I have endured everything that I have in this detention facility for the past 28 months.’ Illustration: Rita Liu/The Guardian
A Google Maps screenshot of the South Louisiana Ice Processing Center (SLIPC) in Basile, Louisiana.
Photograph: Google Maps
A spokesperson for Geo categorically denied the allegations detailed in the complaints.
Photograph: Patrick T Fallon/AFP/Getty Images
Queer and trans immigrants at a detention facility in south Louisiana have alleged that they faced sexual harassment and abuse, medical neglect and coerced labor by staff at the facility, and that they were repeatedly ignored or faced retaliation for speaking out.
In multiple legal complaints, immigrants detained at the South Louisiana Ice Processing Center (SLIPC) in Basile, Louisiana, said they were recruited into an unsanctioned work program that forced them to perform hard manual labor for as little as $1 per day. Detainees also alleged that queer people were targeted by an assistant warden who stalked, harassed and sexually assaulted them.
Three current and former detainees who spoke to the Guardian said that, between 2023 and 2025, they endured months of abuse from an assistant warden named Manuel Reyes and his associates. In their complaints to the Department of Homeland Security (DHS) and Immigration and Customs Enforcement (Ice), the detainees also said that they faced retaliation for reporting the abuse to authorities, alleging that Reyes and other staff beat them and denied them medical treatment.
“I was treated worse than an animal,” said Mario Garcia-Valenzuela, one of the detainees. “We don’t deserve to be treated like this.”
Garcia-Valenzuela, a trans man detained at SLIPC, has alleged that, as part of the unsanctioned work program, Reyes forced him to move heavy cabinets and cinder blocks, and to clean using industrial-strength chemicals without gloves or protective gear. When Garcia-Valenzuela complained of injuries from the work program, he said, Reyes and his associates forcefully stripped him naked and mocked him.
Kenia Campos-Flores, who is trans and non-binary, told the Guardian that they suffered from persistent migraines and chest pain after exposure to cleaning chemicals they were made to use during unofficial, overnight work shifts. Campos-Flores also alleged in a complaint they were persistently sexually harassed by Reyes, who entered their dorm and stole possessions including their boxers.
Another trans detainee, Monica Renteria-Gonzalez, complained that a stripper chemical he was told to use to clean the facility floors seeped through his fabric shoes and burned the skin of his feet. On more than one occasion, while Renteria-Gonzalez was bent over cleaning, he said, Reyes came up from behind and inappropriately touched him. The assistant warden also told Renteria-Gonzalez he was watching the detainee through security cameras, including while he was showering.
A fourth detainee, identified by the pseudonym Jane Doe, is a cisgender, queer woman who said that Reyes forced her to perform oral sex on him on a “near daily basis” between February and May 2024, threatening to kill her if she refused, according to her complaint.
Doe, who was deported to the Dominican Republic in January this year, has chosen not to share her name or speak publicly because she fears that Reyes will make good on his threat to find and harm her, her lawyer said.
Taken together, the detainees’ stories present a troubling pattern of mistreatment and abuse inside SLIPC, their attorneys said. Though the alleged abuse took place across two presidential administrations, advocates worry that conditions inside detention facilities could further deteriorate amid the Trump administration’s present push to arrest and detain a record number of immigrants. Trans and queer immigrants in detention are especially vulnerable, advocates said, given that the administration is also moving to roll back key civil rights protections for LGBTQ+ people in federal custody.
The detainees’ allegations are detailed in four separate administrative complaints filed under the Federal Tort Claims Act, which allows individuals to sue the government for injuries caused by federal employees. The government has six months to adjudicate the complaints, or the claimants could move forward with a federal lawsuit. They were submitted in September by Robert F Kennedy Human Rights, the American Civil Liberties Union (ACLU) of Louisiana and the National Immigration Project. Those groups have also submitted a civil rights complaint to the DHS oversight bodies, including the office for civil rights and civil liberties (CRCL), on behalf of the detainees.
“This was a sadistic late-night work program,” said Sarah Decker, a senior staff attorney with RFK Human Rights. “It was designed to target vulnerable trans men or masculine-presenting LGBTQ people, who [Reyes] coerced into participating.”
When detainees tried to report their abuse, Decker said, Ice officials repeatedly disregarded them. Officials dismissed multiple reports of abuse in accordance with the federal Prison Rape Elimination Act (Prea), Decker said, as well as complaints to the Ice office of inspector general (OIG), the department charged with oversight of Ice.
“These people screamed for help. They filed grievances. They filed complaints under the Prison Rape Elimination Act, they filed verbal complaints through the office of the inspector general. They did everything to get help,” Decker said. “And they were systematically ignored, and complaints were buried.”
The Guardian attempted to locate Reyes though multiple means, including public records and social media searches and were unable to contact him. Reyes is not facing criminal charges for the alleged sexual abuse at the facility.
He is no longer employed at SLIPC, Decker said – he left the facility in July 2024. But, Renteria-Gonzalez and Garcia-Valenzuela, who remain detained at SLIPC, told the Guardian other staff at the facility have continued to retaliate against them, placing them in solitary confinement and denying them full access to medical care.
The DHS and Ice did not respond to the Guardian’s queries about the detainees’ allegations, nor did the agencies address whether any of the detainees’ Prea complaints were investigated.
‘It’s devastating and heartbreaking, everything that they do to us in here’
Located about 90 miles (145km) from the Gulf coast in the rural town of Basile, Louisiana, SLIPC was once a correctional facility. But in 2019, it opened as an Ice detention facility, operated by Geo Group, one of the largest private prison and surveillance firms in the US.
Over the past several years, the detention center, which houses mostly women as well as a few trans people, has attracted a string of allegations of civil and human rights violations, medical neglect and poor hygiene. In 2022, an internal inspection by the office of the immigration detention ombudsman – an independent office within the Department of Homeland Security – found that the facility had insufficient medical staffing, and had been inconsistent in addressing the medical and mental health needs of detainees. A 2025 report by the Yale Law School also found that detainees were “left hungry, cold, and in an atmosphere detainees describe as abusive”.
A Google Maps screenshot of the South Louisiana Ice Processing Center (SLIPC) in Basile, Louisiana. Photograph: Google Maps
“It’s devastating and heartbreaking, everything that they do to us in here,” said Renteria-Gonzalez, who first arrived at the facility in May 2023. “We struggle on a daily basis.”
He said his decision to remain in detention while his immigration case is under review – rather than accept deportation – has been painful.
Renteria-Gonzalez came to the US when he was 12 and has been in the country for 31 years. His eight-year-old daughter is a US citizen. “It is for my daughter and my family that I have endured everything that I have in this detention facility for the past 28 months,” he said. “It’s so that I can make it back home to her.”
Renteria-Gonzalez said Reyes first recruited him to participate in the late-night work program in September 2023, according to his complaint. Reyes would often come into his dorm late at night – at around 2 or 3am – to wake him up for his night shift.
“It’s like he lived [at the detention center] 24/7,” Renteria-Gonzalez told the Guardian.
Each recruit worked alone, during different times or in different parts of the detention facility – meaning they were often alone with Reyes, the detainees allege. During these times, Renteria-Gonzalez said, he would watch them work and probe them with invasive and inappropriate questions. “It made me feel uncomfortable,” he said. “He used to sit on his phone and asked us for personal information to look us up on Facebook and stuff.”
Sometimes, he said, Reyes entered detainees’ dorms late at night for no particular reason, and would take their used underwear and personal hygiene products. On other occasions, Renteria-Gonzalez alleged in the complaint, Reyes would stalk him as he went to and from the showers and ask invasive questions: “And after, he would say: ‘Tell me what were you doing in the shower?’”
Twice, Renteria-Gonzalez said, Reyes came up behind him and touched him inappropriately. Another SLIPC officer, according to Renteria-Gonzalez, began to sexually harass him as well, sending him explicit notes and showing him pornographic images of herself.
“I just felt overwhelmed,” he said. “I thought enough was enough.”
Eventually, he realized he wasn’t alone.
After being detained at SLIPC in February 2024, Garcia-Valenzuela said he also found himself trapped in Reyes’s unofficial work program.
Mario Garcia-Valenzuela. Photograph: Mario Garcia-Valenzuela
Garcia-Valenzuela had fled to the US in 2014 from Mexico, where he was tortured by members of a drug cartel. “I have no choice, that’s why I’m fighting,” he said. “Because I know that as soon as they deport me, I’m going to be handed over to the cartels and I’m going to be tortured and killed – ripped into pieces.”
But in SLIPC he faced a new kind of horror. He alleged that on more than one occasion he was told to move heavy metal filing cabinets back and forth across a room. When he struggled to lift the furniture, Reyes would taunt him, he said, saying: “If you think you are a man, I’m going to treat you like a man.”
In the spring of 2024, Garcia-Valenzuela reported sexual harassment on the basis of his gender, in accordance with Prea. He said he felt targeted due to his gender identity and wanted the fact he is transgender removed from his file, as a measure of protection. But an Ice officer responded that “even if we take off your transgender marker, there is no hiding that you are transgender”, noting Garcia-Valenzuela’s physical appearance, he said. To Garcia-Valenzuela’s knowledge, no follow-up investigation into Reyes was conducted.
Renteria-Gonzalez’s complaints were dismissed as well, Renteria-Gonzalez said.
A spokesperson for Geo categorically denied the allegations detailed in the complaints.
“GEO strongly disagrees with these baseless allegations, which are part of a long-standing, politically motivated, and radical campaign to abolish ICE and end federal immigration detention by attacking the federal government’s immigration facility contractors,” said Christopher V Ferreira, a Geo group spokesperson.
Ferreira added that “GEO has comprehensive policies in place for the reporting and investigation of all incidents that occur at the Center, including instances of assault and/or sexual assault. These policies are governed by standards and requirements established by the US Department of Homeland Security.”
Geo did not respond to questions about Reyes’s employment status at SLIPC.
Harsh retaliation
The detainees who filed complaints against Reyes and other SLIPC staff said that they faced harsh retaliation for doing so.
When Jane Doe filed a Prea complaint with Ice using a paper form and through the phone hotline, detailing that Reyes had sexually assaulted her, she received no response, according to her legal complaint.
But afterwards, Reyes redoubled his efforts to stalk her, the complaint alleges – and forced her to perform oral sex on him, saying he had her cornered in the facility’s “camera blind spots” where no one would see them.
When she attempted to resist, Reyes told her he had found her mother’s home address in the Dominican Republic, Doe alleges in the complaint, and told her that if she were deported, he would follow her to her family’s residence where “you won’t have any protection”.
A spokesperson for Geo categorically denied the allegations detailed in the complaints. Photograph: Patrick T Fallon/AFP/Getty Images
Jane Doe said Reyes and other staff also blocked her from accessing medical treatment for her epilepsy, even as her seizures became more severe and frequent during her time in detention, the complaint states. He repeatedly cornered Doe as she was en route to the medical center to receive treatment, and told her he would watch her on cameras while she was receiving medical evaluation. On one occasion, he told Doe he was “masturbating to her because he saw her body in medical condition when she was in an observation cell”, the complaint alleges.
“We feel so vulnerable, impotent,” Renteria-Gonzalez said.
After he reported that Reyes had sexually assaulted him, Renteria-Gonzalez said, Reyes burst into his housing unit and yelled, “You should have never put my name on it!”, in reference to the complaint to Ice. Renteria-Gonzalez said he was then placed in solitary confinement for two weeks.
After Renteria-Gonzalez reported harassment from another officer, his complaint was dismissed as “unsubstantiated” and the officer came back and told him: “They can’t do nothing to me,” according to the complaint.
Meanwhile, Garcia-Valenzuela said he was repeatedly sent to solitary confinement, he believes in retaliation for speaking out. He said staff at the detention center falsely reported that he had attempted self-harm, and needed to be placed under suicide watch, even though he had not in fact tried to hurt himself.
At one point, while Garcia-Valenzuela was in the medical isolation unit, officers delivered him a meal that consisted of a few potatoes and a few grains of cereal. There was no spoon provided, he said, and there was a note that instructed him to eat it “like a dog”.
Shortly after that incident, he said, a doctor at the facility suddenly – without explanation – stopped providing him access to medication for hand pain that had been exacerbated by his working in Reyes’s night-shift program.
He has avoided making further complaints. He tries not to speak to or make eye contact with staff, and avoids leaving his dorm. He limits trips to the restroom, he said. And rather than go to the cafeteria to warm up his food and eat, he takes his meals cold, and dines in bed. “I have to stay in the back-most corner of my bed, and eat there,” he said.
“I don’t ever feel at ease.”
Trans people in federal custody under threat
The allegations of abuse at SLIPC come at a time when the health and safety of trans people in federal custody is especially under threat, advocates say.
On the first day of his presidency, Donald Trump unveiled a flurry of executive actions targeting trans rights, rolling back anti-discrimination protections and mandating that people in immigration detention be placed in facilities based on their sex assigned at birth.
On 16 January – the last day of Joe Biden’s administration – Ice reported that 47 trans people were in Ice detention facilities around the country and that 69 had been arrested since the start of the fiscal year. As soon as Trump took office, the agency began omitting data on the number of transgender people in immigration detention from its reports.
“The government is essentially refusing to acknowledge the existence of trans people, let alone their humanity,” Decker of RFK Human Rights said.
Although a federal judge has blocked enforcement of Trump’s ban on transgender healthcare in federal prisons, Decker told the Guardian that inside detention centers, guards and staff have been emboldened to deny healthcare to trans clients, or retaliate against them for requesting care.
“I worry that the situation will only get worse from here for trans people,” she added.
The administration also closed the civil rights division of the DHS, as well as the ombudsman office overseeing immigration detention, arguing that the staff in these congressionally mandated divisions were “internal adversaries that slow down operations”.
The divisions included employees tasked with regularly visiting detention centers, investigating complaints and preparing reports for Congress. Detainees facing discrimination, neglect and abuse now have even fewer options for recourse, Decker said.
LGBTQ+ Americans consider move to Canada to escape Trump: ‘I’m afraid of living here’
Read more
It’s a scary, difficult moment to speak out, said Campos-Flores, a 37-year-old single parent of two children who came to the US from El Salvador when they were 11 years old.
During the seven months that Campos-Flores was detained at SLIPC, they would call their parents every day, just to reassure them that they were still alive. Periodically, they would beg their family and their lawyer to find ways to get them out. “I asked them to try to book me into another facility,” they said. “It was too much – just too much.”
In November 2024, they were deported – and immediately they felt a sense of relief to be freed from Reyes, they said. But they couldn’t stay away from their children, who are US citizens – so they crossed back into the US and were again apprehended.
They are currently detained at a different correctional facility in Louisiana, serving a criminal sentence for illegal re-entry. But after finishing their sentence, it is likely they will be transferred back to SLIPC before deportation – and face the same officers who harassed them, or ignored their complaints.
“But I have my 12-year-old son. He is also gay, he likes boys, and I don’t want him to experience anything like what I have experienced,” they said. They want to fight for his rights, too, they said.
Fox host tries to force him into a hole so she can bash him with bigotry. He doesn’t fall for it. Hugs.
tRump / Rubio are desperately trying to drum up a war with Venezuela over their oil. The US handpicked successor to Maduro admitted she would give up the rights to the oil reserves to the western oil companies first thing. Venezuela has more oil than Saudi Arabia. That is why the US crippled the Venezuela economy in an attempt to get hat oil for our own. Maduro wants to use the money for the people, he wants to help the indigenous people, he wants to destroy the class structure that existed when he was growing up. The white people were treated better than the native brown people, he wanted to change that to where everyone is equal. People who are used to privilege react badly when everyone gets the same privilege. Hugs
This next video talks about the “young republicans” who are anywhere from 18 to 40 and these racist bigoted republicans have important positions in state and federal government. These republicans threatened to rape their enemies, and praised Hitler. Hugs
The clip below talks about Chuck Schumer and his actions before the shutdown and after. The democrats have a history of not standing up and taking action. The base of the party is glad the leaders are now taking concrete actions. Hugs
This last one is just for fun. It is a comedian who acts / talks like Cuomo to his face. Hugs
Despite repeatedly promising not to cut Social Security, the Trump Administration is reportedly preparing a proposed rule that could reduce the share of applicants who qualify for Social Security Disability Insurance (SSDI) by up to 20 percent, according to an Urban Institute report that cites writing by a former Trump Administration official and interviews with former staff at the Social Security Administration (SSA). This would be the largest cut in SSDI history.
SSDI is an integral part of Social Security. It provides essential benefits to workers who cannot support themselves through earnings due to severe and long-lasting disabilities that significantly impede their ability to work, and it helps to prevent beneficiaries and their families from experiencing poverty.
The rule would make it much more difficult to qualify for both SSDI and Supplemental Security Income (SSI). Because it would dramatically change the eligibility criteria for older applicants, the losses among people over age 50 would be much deeper.
The rule is likely to be the largest-ever cut to Social Security Disability Insurance. A 20 percent cut in the share of applicants who qualify for SSDI would be larger than any previous change to the program. It would be even larger than the Reagan-era disability cuts, which the Reagan Administration was forced to reverse amid fierce opposition from governors, courts, beneficiaries, and advocates. According to an Urban Institute analysis, even a cut half the size of what the Trump Administration is considering would mean 750,000 fewer people would receive SSDI benefits within ten years. In addition to reducing the share of applicants who receive benefits, some current beneficiaries could see their benefits taken away when their eligibility is reviewed.
The rule would particularly hurt older workers. Like the rest of Social Security, SSDI serves largely older people; nearly 80 percent of disabled workers are aged 50 or older. SSDI benefits provide vital support to people whose careers are cut short by severe medical impairments. The rule is expected to target older applicants already determined to have significant medical impairments by discounting the barriers they face due to their age in continuing to do substantial work — despite the law’s requirement that the Social Security Administration (SSA) consider how age, education, and skills might make working harder, in addition to considering health conditions.
It’s already difficult at any age to qualify for disability benefits, given their stringent rules. Research shows applicants whose impairments are not severe enough to qualify for SSDI fare poorly in their attempts to return to work — especially if they’re older. Rejecting more older applicants will cause more hardship for people who would be eligible for benefits under the existing rules.
The rule will likely cause disproportionate harm to people living in the South and Appalachia. Some states have a higher share of people receiving disability benefits, particularly those with more older workers with fewer years of formal education, and who are more likely to have worked in physical jobs like manufacturing or mining. That is true of many Southern and Appalachian states, as well as Maine and the Rust Belt states of Michigan, Ohio, and Pennsylvania. The proposed rule drafted during the first Trump Administration would reportedly change the way SSA considers education as well as age, and because residents of these states are on average older and less educated, these changes will hit them doubly hard.
In addition to cutting Social Security and SSI, the rule would threaten retirement security, access to health care, and other supports. Workers who become disabled and qualify for SSDI are significantly worse off in retirement: they are poorer, experience more hardship, and have lower savings. Disabled workers will fare even worse in retirement if their eligibility for disability benefits is stripped. They would be forced to spend any retirement savings faster and claim their Social Security retirement benefits at a younger age, permanently reducing their — and possibly their family’s — monthly Social Security retirement benefits by up to 30 percent. For hundreds of thousands of older people, this rule would create long-term financial insecurity as they age.
In addition, applicants who do not qualify for disability benefits may face significant challenges accessing health care. SSDI recipients typically receive Medicare 24 months after they begin to receive benefits; if someone no longer qualifies for these benefits, they won’t be able to get Medicare until they turn 65. And, SSI recipients receive Medicaid, so those who lose SSI benefits may also lose Medicaid (particularly in states that have not adopted the Medicaid expansion). Most rejected applicants under the new standard will have very significant medical impairments, and many will struggle to access health care without those benefits — particularly after the steep Medicaid cuts in the Republican megabill.
Finally, restricting eligibility for disability benefits will make it more difficult for rejected applicants to access other key supports, such as food assistance, which has increasingly strict time limits for most non-elderly individuals without younger children who are not receiving disability benefits. New Medicaid work requirements could also pose significant impediments to people who lose disability benefits.
This rule is the latest in a series of harmful actions by the Trump Administration that threaten access to Social Security. This year, the Administration has forced SSA through a radical downsizing that has disrupted services for the largely older and severely disabled people who rely most on the agency, indiscriminately pushing out 7,000 workers in the largest staff cut in SSA’s history. This realignment has resulted in fewer staff serving Social Security applicants and beneficiaries, and huge cuts to staff supporting the agency’s customer service mission. These cuts have been coupled with inexplicable new restrictions — some of which have already been partially rolled back — for how the public can engage with SSA for assistance, creating additional access barriers.
At the same time, the Administration is working to advance changes that would make it harder for hundreds of thousands of eligible people to receive or continue receiving SSI, creating additional red tape for beneficiaries and more work for depleted and overburdened SSA staff.
I recently transferred to the rehab center, which is just across the street from the hospital. Today I took a cognitive test, I took a speech pattern test, and I took a physical test. Every day from here on out, I will be taking a physical test, which we call PT. They usually wanna work people till they wanna quit, but they haven’t had that problem with me yet, not because I’m super amazing or awesome, but because I really want to beat this shit as quickly as I can.
My friend Melissa Colombo came by and brought me some clothes. Nobody can go on Facebook and ask people to bring them shorts, T-shirts, and underwear while they’re in a rehab center, but I can. Hell, I once got people to send me self-addressed stamped envelopes for messed-up business cards. But I sent out a request on Facebook for someone to bring me some shorts and T-shirts to the rehab center. All I had this morning was just a road in the hospital, and my ass was hanging out.
A few people offered to ship me stuff, but that wasn’t the issue. I have money. I could easily order something. But I need something now because, let me put that again, my ass was hanging out. So my friend Melissa brought me some clothes. Funny thing is, someone else went ahead and quickly ordered me some stuff, and that was Leslie Elliott.
I want to thank Melissa and Leslie for literally saving my ass.
The next 10 days are going to be more PT. I am expected to be in this place for at least 10 days. After that, I’m expected to go home. The thing is, I live in a second-level apartment, and I want to be able to walk into my apartment and take care of myself again. Unfortunately, I’m nowhere close to that yet. Walking, taking steps, things are extremely difficult right now, and even grabbing things is impossible, but I am further today than I was yesterday.
If you have donated to me either by becoming a paid subscriber to my Substack, or donated through PayPal, or donated through Venmo, or donated through Zelle, and I have not sent you a message, please accept my apologies. I want to thank everybody who has supported me through this. The outpouring of support has blown me away. In fact, it’s blown away the entire cartooning community. We are all very impressed and overwhelmed by your support, especially me. I just wanna say thank you. I’m never going to stop saying thank you.
And on that note, I was just visited by a former photographer from the Free Lance-Star, Suzanne Carr Rossi. She brought me pants.
And now the Facebook updates from the past few days.
Today, October 16, 2025
Remember when Donald Trump took that cognitive test and bragged about it? Remember that he had to repeat “person, woman, man, camera, TV”. Trump said. “They said nobody gets it in order, it’s actually not that easy. But for me it was easy. And that’s not an easy question.” He is right.
It’s not an easy question when you have to answer five minutes later.
It’s not easy when the question is “bridge, Sarah, justice, banana.” It’s not easy when you have to remember photos that include car keys, a comb, and a helicopter five minutes later.
It’s not easy when you have to remember letters and numbers in the sequence of 1, A, 2, B, 3, C, 4, D, etc, to ten.
It’s not easy to count backwards from 20.
It’s not easy to have to draw a clock and other shapes with your left hand when you’re handed and your right hand is kind of dead from a stroke.
It’s not easy to do any of the stuff after having a stroke, but I did it. The thing is, nobody told me I was great or amazing for it. Sicophants didn’t fawn over me for it. Nobody threw a parade for me because I remembered five words. Idiots didn’t go until late-night TV to tell me I was a genius for it.
Donald Trump wants you to treat him like a baby for remembering five words.
Donald Trump never suffered from a stroke.
So why was Donald Trump given this cognitive test?
Who knew that my stroke would become part of my research?
October 16, 2025
Ok, Peezeheads!!! Who wants to volunteer to help out a stroke victim, and possibly an opportunity to see my ass?
I am at Encompass in Fredericksburg. I need someone to bring me a few button-up shirts. I can’t use a T-shirt because my shoulder is messed up from the stroke. I also need a pair of shorts. I just need athletic shorts, nothing with buttons or belts, or zippers. 
I could also use some underwear.
At this time, I am still wearing the gown from the hospital, and my ass is hanging out. Fortunately, the entire nursing staff has told me that my butt is not too hairy, but maybe they’re just being nice. 
Update: I am only asking local people to help. I need this stuff today, not delivered by Amazon. Thank you.
Update update: Melissa Colomboto the rescue, and then Leslie Elliott, and my friend Suzanne.
October 15, 2025
So many people have touched me this week, and I’ll never be able to you how much it means to me.
As I was being rolled out on a gurney to be taken to the rehab center, an old friend I hadn’t seen in nearly a decade was waiting outside my hospital room to see me.
I want to cry. I love you, Rhonda.
October 15, 2025
I had an MRI this morning after the procedure scan my heart. They were looking to see if there was a hole or any other abnormalities in my heart that may have caused the stroke. As it turns out, there’s nothing wrong with it.
But the MRI was brutal. You can’t move, your back hurts, you don’t know when it’s going to end, you are continuously being asked to hold your breath, and they’re playing 90s music made by other people. Instead of Pearl Jam, you’re getting Pearl lame.
It’s time to go. They want more blood.
October 15, 2025
I am being moved tonight to a rehab facility. I think this is good news. 
October 15, 2025
One of my nurses was training another nurse this morning. Just as the trainee was applying alcohol to my skin, in order for me to inject myself with insulin (yes they are making me inject myself), I decided let out a little scream. AAAAAGH! The trainee jumped, and the other nurse laughed her ass off, and said that was great.
They both said that they’re going to remember me.
Damn straight.
This is the GoFundMe set up by Kevin Necessary and Jack Ohman
This is a cartoon drawn by John Buss.
How to draw Peezy by Dave Whammond, and he’s trying to get more cartoonists to join in. I hope it happens because I would love to see more of my colleagues’ renditions of our favorite pizza.
I am not trans even though I have been asked because of my super strong support of trans people. I have lost friends who wouldn’t accept trans people using a public bathroom with them even though all private functions happen in enclosed little stalls. I do have distant family members who are trans and fully supported by family. More important I can clearly see the same negative vile things said about trans people are the same things pushed against gay people when I was a struggling gay teen being pushed by the same groups on the same ideas of victimhood. They were mostly driven by hyper Christian Nationalist religious groups and those who demanded that traditions along with society never change from when they were young and happy. These same groups and feelings are in play against trans people. They are simply the homosexual aids scare of the 1980s. Just as I as a young gay person needed allies and support so do trans people today. Please give as much vocal and upfront support for trans people you can. It is easier to make progress as a society if we don’t have to undo hateful laws outlawing our very existence. Hugs

‘It is for my daughter and my family that I have endured everything that I have in this detention facility for the past 28 months.’ Illustration: Rita Liu/The Guardian
A Google Maps screenshot of the South Louisiana Ice Processing Center (SLIPC) in Basile, Louisiana.
Photograph: Google MapsA spokesperson for Geo categorically denied the allegations detailed in the complaints.
Photograph: Patrick T Fallon/AFP/Getty Images